Your brain runs on a clock that needs sunlight to stay accurate
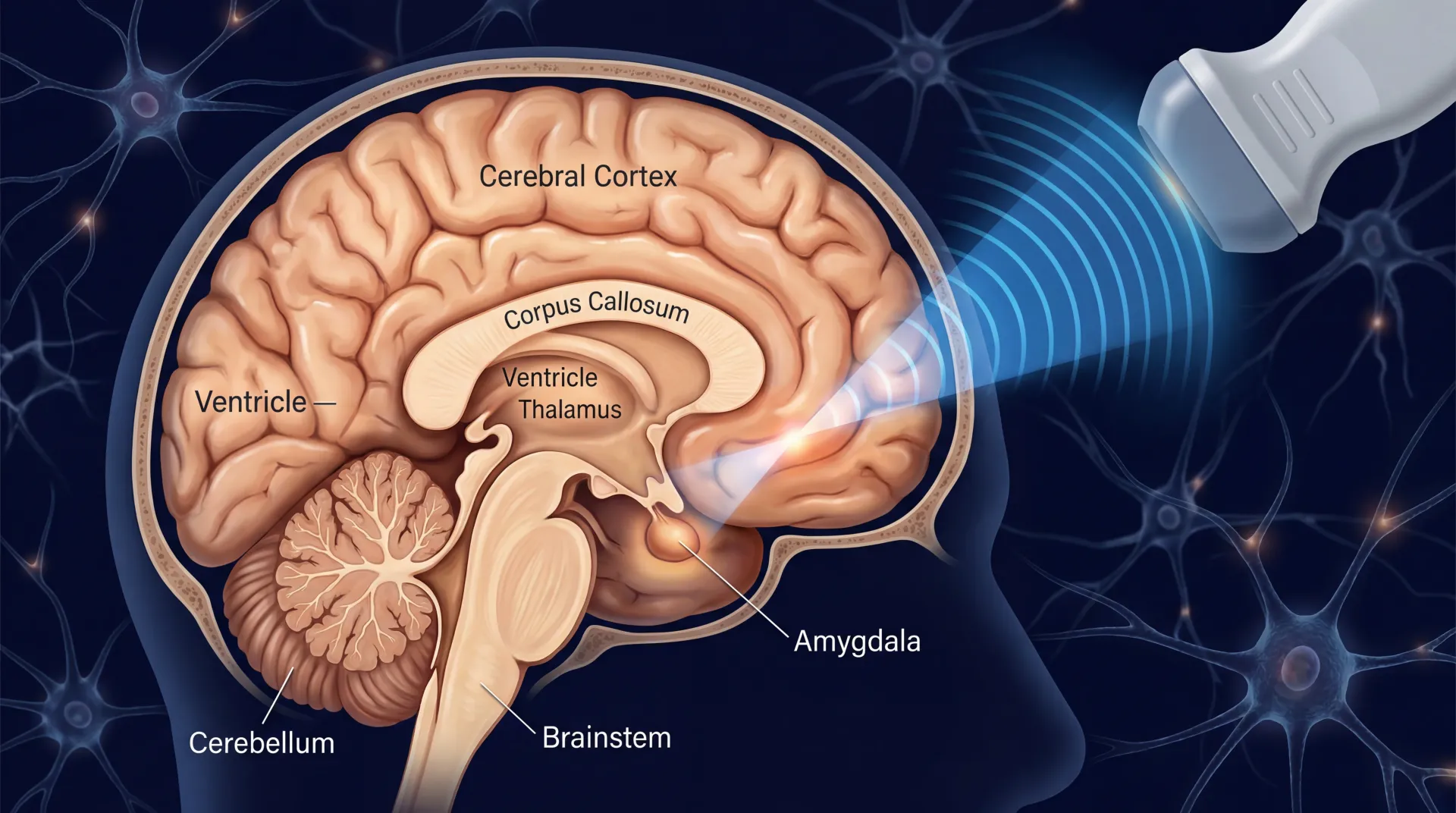
Deep inside your hypothalamus sits a tiny cluster of neurons called the suprachiasmatic nucleus, or SCN. This is your body's master clock. It orchestrates when you feel sleepy, when cortisol spikes to wake you up, when your gut ramps up digestion, and when your body temperature drops at night. The SCN keeps all these rhythms humming on a roughly 24-hour cycle, but it can't do it alone. It needs a daily calibration signal, and that signal is light entering your eyes.
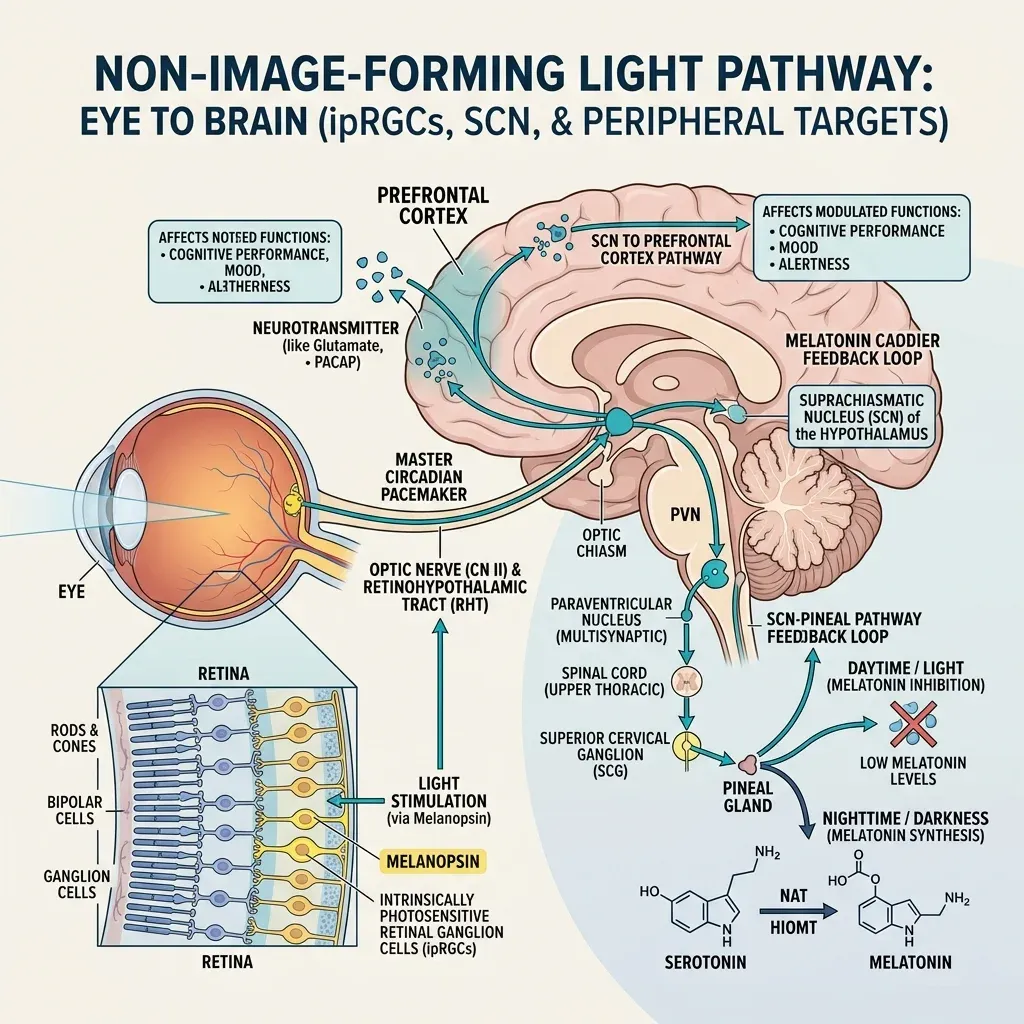
Think of the SCN like a wristwatch that loses a few minutes each day. Without regular adjustment, it drifts. Sunlight is the mechanism that resets it every morning. The resetting happens through a specific class of retinal cells discovered in the early 2000s: intrinsically photosensitive retinal ganglion cells, or ipRGCs. These cells contain a photopigment called melanopsin, and unlike the rods and cones you use for vision, ipRGCs don't help you see. Their job is to measure ambient light intensity and relay that information directly to the SCN through a dedicated neural highway called the retinohypothalamic tract. Melanopsin absorbs light most efficiently in the blue wavelength range, around 480 nanometers.
The clock-resetting function is well established. What caught researchers off guard was finding additional neural pathways running from these same retinal light sensors to the prefrontal cortex, the brain region that regulates mood and higher-order cognition. Dr. Richard Schwartz, an associate professor of psychiatry at Harvard Medical School, has noted that "beyond setting our circadian clock, light exposure also seems to affect higher-functioning areas of the brain." This dual action helps explain why bright light can influence mood even in people whose circadian timing is fine.
The serotonin connection adds another layer. A PET imaging study of 88 individuals in Toronto led by Praschak-Rieder and colleagues found that serotonin transporter binding potential in the brain increased during fall and winter compared to warmer months. More transporter activity means more serotonin gets vacuumed out of the synaptic cleft, leaving less available to signal between neurons. In people with SAD, this seasonal increase was even more pronounced. After bright light therapy, transporter activity dropped back to normal levels, according to a follow-up study by Willeit and colleagues.
Light also influences serotonin turnover directly, with the lowest rates of turnover occurring in winter and faster turnover during periods of greater light exposure. And there's evidence that bright light enhances dopaminergic transmission in certain brain regions, though this pathway is less well-studied. One study even tested whether BLT could work through the skin rather than the eyes by administering light to the back of the knee. It had zero effect on depressive symptoms, confirming that the eyes are the required entry point for light's antidepressant action.
For anyone with SAD, the leading explanation of what goes wrong is the phase-shift hypothesis. As days shorten in fall and winter, the circadian clock begins to drift later relative to the sleep-wake cycle. Researchers at the National Institute of Mental Health have described this as essentially a winter-long jet lag, where internal timing and external schedule fall out of alignment. Morning bright light treatment corrects this by pushing the clock earlier, a process called phase advance. The practical upshot: if your brain is getting a 6 AM wake-up signal at 8 AM, a morning light box can pull that signal back to where it belongs.
61% remission in SAD patients, and the numbers for non-seasonal depression are catching up
The evidence for bright light therapy in seasonal affective disorder has been accumulating for four decades, starting with Norman Rosenthal's landmark 1984 study that first described both the condition and its response to light. The data at this point is unambiguous. Two meta-analyses covering eight randomized controlled trials with 703 total participants confirmed that bright light therapy outperforms control conditions for SAD, and both the American Psychiatric Association and the Canadian Network for Mood and Anxiety Treatments now list it as a first-line treatment.
One of the most striking individual trials came from Eastman and colleagues, who found that 61% of 33 patients with SAD reached full symptom remission after four weeks of bright morning light, compared to just 32% of the 31 patients who received a placebo condition. Remission here was defined strictly: a 50% or greater reduction on the SIGH-SAD scale plus a final score of 8 or below. That nearly two-to-one remission advantage held up to statistical scrutiny.
For both seasonal and nonseasonal depression, the effectiveness of light therapy is approximately the same as antidepressant medications, or popular forms of psychotherapy such as cognitive behavioral therapy. Each reportedly improves symptoms in between 40% to 60% of people. - Dr. Richard Schwartz, Harvard Medical School
What most people miss: bright light therapy also works for non-seasonal depression. A 2024 systematic review and meta-analysis published in JAMA Network Open analyzed 11 randomized controlled trials involving 858 patients with non-seasonal depressive disorders. The BLT group achieved remission at a rate of 40.7% compared to 23.5% in controls, with an odds ratio of 2.42. Response rates were even more pronounced: 60.4% vs 38.6%. The American Academy of Family Physicians reviewed this same evidence in 2025 and assigned it a Level of Evidence rating of 1a, the highest tier.
An earlier and larger meta-analysis by Perera and colleagues, covering 20 RCTs with 881 participants, found a standardized mean difference of -0.41 in favor of light therapy for non-seasonal depression. That effect size is moderate and clinically meaningful, though the authors noted significant heterogeneity between studies and high risk of bias in some trials.
Then there's the direct comparison with antidepressant medication. A meta-analysis of seven direct comparison trials involving 397 participants found no significant difference between light therapy alone and antidepressant drugs alone (SMD = 0.19, p = 0.17). But the combination of light therapy plus medication was significantly better than medication alone, with an effect size of 0.56. That combination advantage held up specifically in the non-seasonal depression subgroup.
Dr. Raymond Lam at the University of British Columbia ran the cleanest head-to-head trial. His eight-week randomized, double-blind trial of 122 outpatients found that BLT plus fluoxetine produced a mean MADRS improvement of 16.9 points versus 8.8 for fluoxetine alone (p = 0.02). The effect sizes were 1.11 for the combination, 0.80 for BLT alone, and just 0.24 for fluoxetine alone. In that trial, a light box outperformed one of the most prescribed antidepressants in the world.
Not everyone responds equally. Patients with atypical depression features respond better to light therapy. Robert Levitan, writing in the Journal of Psychiatry and Neuroscience, noted that carbohydrate craving and hypersomnia predict a robust response to BLT, while melancholic symptoms like insomnia and weight loss are generally less responsive. This makes biological sense given that atypical depression has stronger circadian components.
The evidence-based morning protocol: 30 minutes that can shift your chemistry
Three decades of research have converged on a protocol that barely varies from one clinical guideline to the next.
| Parameter | Recommendation | Source basis |
|---|---|---|
| Intensity | 10,000 lux | Standard across all major clinical guidelines |
| Duration | 30 minutes per session | 5,000 lux-hours optimal dose (10,000 x 0.5h) |
| Timing | Within first hour of waking, before 8 AM | Mayo Clinic, multiple RCTs |
| Distance | 16-24 inches (41-61 cm) from face | Mayo Clinic, device-specific |
| Angle | ~30 degrees from line of gaze; eyes open, don't stare | Campbell et al. |
| Frequency | Daily, including weekends | Levitan |
| Expected onset | 3-7 days | Multiple sources |
The logic behind the 10,000 lux standard is straightforward: it's the dose that allows for the shortest practical session. The therapeutic dose is actually measured in lux-hours. As Levitan explains, 5,000 lux-hours is the sweet spot. You can get there with 10,000 lux for 30 minutes, 5,000 lux for an hour, or 2,500 lux for two hours. Most people find 30 minutes far more sustainable than two hours, which is why 10,000 lux devices dominate the market.

Timing matters more than many users realize. Morning light is optimal because it generates a phase advance of the circadian clock, correcting the delayed rhythms that underlie both SAD and many cases of non-seasonal depression. Maruani and Geoffroy's clinical guidelines recommend early morning treatment around 8 AM, with chronotype taken into account. If you're naturally an extreme early bird, you might need to start earlier; if you're a night owl (which many depressed patients are), the timing should follow your natural wake time rather than a fixed clock time.
The position of the light box is another detail that affects real-world results. The device should sit at or slightly above eye level, angled downward so the light enters your eyes at roughly 30 degrees from your line of gaze. You should never stare directly into the light. The practical setup most researchers describe involves placing the box on a table while you read, eat breakfast, or work on a computer. This passive exposure is the whole point: the therapeutic benefit comes through your open eyes even when you're not looking at the device.
Distance is not negotiable. Light intensity follows the inverse square law, meaning that doubling your distance from the light source cuts the intensity to one quarter. A device rated at 10,000 lux at 12 inches delivers only about 2,500 lux at 24 inches. This is why the distance specified by the manufacturer is the most important number on the box.
| Lux level | Duration needed | Distance (typical) | Equivalent to |
|---|---|---|---|
| 10,000 lux | 30 minutes | 12-14 inches | Bright overcast day |
| 5,000 lux | 60 minutes | 18-24 inches | Standard office lighting x10 |
| 2,500 lux | 2 hours | 24-36 inches | Well-lit retail store |
Bright light therapy works faster than antidepressants. While SSRIs typically require several weeks to show clinical effects, BLT can produce measurable improvement within the first three to seven days. Levitan notes that this rapid onset means treatment can be started when symptoms emerge rather than as a preventive measure, though for SAD patients, beginning a few weeks before the usual seasonal onset can head off symptoms before they arrive.
What actually matters when choosing a 10,000 lux light box
The light therapy device market is unregulated. The FDA does not regulate light boxes for SAD treatment, which means any manufacturer can slap "10,000 lux" on a product without standardized testing. That puts the burden of verification on the buyer.
Alfred Lewy, one of the first researchers to describe SAD in 1980, put it bluntly in an interview with Wirecutter: "I insist, absolutely, that any reputable, reliable manufacturer has to tell the consumer what the distance it should be from the eyes to achieve 10,000 lux. If a light box doesn't have that information, I wouldn't use it."
Five specifications separate a therapeutic device from an expensive night light.
Light face size. Bigger is better, and this is the single most overlooked factor. Norman Rosenthal, the psychiatrist who coined the term SAD, noted in his book Winter Blues that the lights used in almost all research studies had an illuminated surface at least about one foot square. A larger light face means more consistent lux delivery even if you shift slightly in your chair. Compact desk lamps with 6-inch faces can technically hit 10,000 lux, but only at extremely close range, which most people find impractical.
Distance for 10,000 lux. The distance at which a device actually delivers its rated lux is the number that determines your daily experience. A lamp offering 10,000 lux at 14 inches lets you sit comfortably at a normal desk setup. One that requires 6 inches of distance means you're essentially pressing your face against it.
UV filtering. All reputable devices filter ultraviolet light. The Yale Winter Depression Research Program recommends broad-spectrum white light as the best balance of effectiveness and safety. While blue light has stronger circadian effects, Yale notes it is also more toxic to the retina and currently recommends against blue-only devices.
Color temperature. Measured in Kelvin (K), this determines how warm or cool the light appears. Lower numbers (3,500K) produce a warm, yellowish glow; higher numbers (6,500K) produce a cool, blue-white tone similar to noon daylight. Research hasn't definitively shown one is more effective than the other, but comfort affects compliance, and compliance determines results.
Timer function. A built-in timer that shuts off after 30 minutes is a convenience that removes one more friction point from daily use.

| Device | 10,000 lux at | Light face | Color temp | Type | Approx. price |
|---|---|---|---|---|---|
| Carex Day-Light Elite | 12-14 inches | 15.5 x 13 in | 4,000K | LED | $120-150 |
| Northern Light Technologies Boxelite | 14 inches | 15.5 x 12.5 in | 3,500K | Fluorescent | $150-180 |
| Beurer TL95 | 10 inches | 12 x 15 in | 6,500K | LED | $130-160 |
| Verilux HappyLight Luxe | 6 inches | 9 x 6 in | 3,500-5,000K | LED | Under $100 |
Most clinically tested light boxes fall in the $100 to $200 range. That's a fraction of the cost of a month of psychotherapy or a year of antidepressant medication, and unlike pharmaceuticals, a quality light box should last for years. Health insurance rarely covers the purchase, though the number of private insurers viewing light therapy as "medically appropriate" for patients meeting SAD criteria has been increasing.
One practical tip from the Yale Winter Depression Research Program: free smartphone apps can measure lux output using the front-facing camera. You can verify that your device actually delivers 10,000 lux at your preferred sitting distance, and check how far off-center you can move while still receiving a therapeutic dose.
Beyond winter: why light therapy works twelve months a year
Most people put their light box away in April. The research suggests they shouldn't. non-seasonal depression patients often have circadian abnormalities including irregular sleep-wake patterns, altered social rhythms, diurnal mood swings, and disrupted circadian hormone patterns. If the underlying mechanism involves circadian misalignment, it doesn't matter whether it's December or July.
The clinical data backs this up. The 2024 meta-analysis found BLT effective as an adjunctive treatment for non-seasonal depression with an odds ratio of 2.42 for remission, and the subgroup analysis from the head-to-head comparison with antidepressants confirmed this superiority specifically in the non-seasonal depression subgroup (SMD = 0.55, p = 0.005). The AAFP reviewed this evidence in July 2025 and gave it the highest evidence rating.
Bright light has been successfully applied to circadian phase disorders associated with jet lag and shift work, making it a practical tool for anyone whose schedule regularly clashes with the light-dark cycle. Night shift workers, frequent travelers across time zones, and people with delayed sleep phase disorder can all use timed light exposure to push their internal clock in the needed direction.
Maruani and Geoffroy, in their clinical guidelines published in Frontiers in Psychiatry, go further, arguing that light acts as a therapeutic mood stabilizer during remission by stabilizing sleep and circadian rhythms. For people with recurrent depression, this maintenance function could be as valuable as the acute antidepressant effect. The protocol for non-seasonal use differs slightly from the SAD protocol: the recommended approach is a slower titration, starting at lower durations and increasing by 15 minutes per week, with typical onset of response at 2-5 weeks rather than the 3-7 days seen in SAD.

For perspective, consider the outdoor comparison. A bright sunny day delivers about 50,000 lux, while a gray overcast day sits around 10,000 lux. Most indoor environments deliver 100-500 lux. If you work indoors under artificial light and commute in the dark hours, your brain may be getting less light signal than it needs regardless of the calendar. A 30-minute morning session with a light box can bridge that gap year-round.
The population that may benefit most from year-round use are people whose depression has never fit the seasonal pattern but who do notice that their mood, energy, or sleep fluctuates with their light exposure. The finding that BLT combined with fluoxetine produced an effect size of 1.11, versus 0.24 for fluoxetine alone, was demonstrated in a non-seasonal sample and has shifted clinical thinking about when and for whom light therapy makes sense.
Who should be careful, and what actually goes wrong
The side effect profile of bright light therapy is mild by any standard. In the most rigorous study on the subject, Botanov and Ilardi conducted a placebo-controlled trial with 213 healthy young adults, comparing a single 30-minute session at 10,000 lux against a dim red light placebo. The result: no significant difference in any reported side effect between the two groups. Eye strain and blurred vision increased slightly in both groups equally, suggesting that sitting still and reading for 30 minutes under any light source produces some eye fatigue.
The side effects that do appear in clinical populations with depression are headache, eyestrain, and nausea, though these are consistently described as mild and transient across all major reviews. The Botanov study raises the possibility that some commonly reported side effects in depressed populations reflect depressive interpretive biases rather than the light itself, since depressed individuals tend to interpret physiological changes more negatively.
Bipolar disorder is the one population where real caution is warranted. Light therapy can trigger hypomania or mania in susceptible individuals, and this risk must be taken seriously. However, the data is more reassuring than the warnings suggest. A systematic review by Benedetti covering 799 treated patients found that the rate of manic switch after morning bright light therapy was close to 4.2%, which is essentially the same rate expected during placebo treatment of bipolar disorder. By comparison, antidepressant drugs trigger manic switches at rates of 15-40%. For bipolar patients, the evidence supports midday rather than morning exposure, a slower dose titration starting at 15 minutes and increasing weekly, and always using BLT alongside a mood stabilizer.
| Concern | What the evidence says | What to do |
|---|---|---|
| Eye damage | Ophthalmological studies show no damage from 10,000 lux devices | Use UV-filtered devices; consult eye doctor if over 65 |
| Bipolar mania | ~4.2% switch rate (same as placebo) | Use midday timing, slow titration, mood stabilizer |
| Retinal conditions | Contraindicated without ophthalmologist clearance | No BLT with macular degeneration, diabetic retinopathy, glaucoma |
| Photosensitizing meds | UV-filtered devices emit no UV, but caution advised | Check with prescriber if on fluoroquinolones, tetracyclines, NSAIDs |
| Headache/eyestrain | Mild, transient, not significantly different from placebo | Increase distance or reduce session to 15 min temporarily |
Specific contraindications where light therapy should be avoided or used only under medical supervision include: macular degeneration, glaucoma, cataracts, retinitis pigmentosa, and diabetic retinopathy. The Yale Winter Depression Research Program also recommends that anyone over 65 consult an eye doctor before starting BLT, and Levitan suggests ophthalmologic assessment every 2-3 years for long-term users, particularly those at higher risk for eye disease.
The medication interaction worth knowing about involves photosensitizing drugs: fluoroquinolone antibiotics (ciprofloxacin, levofloxacin), tetracyclines (doxycycline), sulfonamides, antimalarials (hydroxychloroquine), and some NSAIDs (naproxen, piroxicam). Properly designed light boxes emit no UV light, and the photosensitivity reactions from these medications are primarily UV-mediated, but the Yale program still advises caution. If your physician has told you to avoid sun exposure because of a medication, discuss BLT use before starting.
One additional note from Yale that deserves mention: like all antidepressant treatments, light therapy can increase energy and agitation before mood fully improves, and in rare cases this gap could be associated with suicidal ideation. This is the same activation risk seen with SSRIs during the first weeks of treatment. The program emphasizes that light treatment should be done under the supervision of a qualified clinician, not as a self-prescription.
Frequently Asked Questions
Can I use a regular bright lamp instead of a dedicated light therapy box?
Standard household lamps typically produce 200-500 lux at a reading distance, which is nowhere near the 10,000 lux needed for therapeutic effect. Even a very bright room rarely exceeds 1,000 lux. Dedicated light therapy devices are engineered to deliver a concentrated, UV-filtered beam at a specific distance. Robert Levitan warns against homemade setups, which may lack appropriate brightness and UV filtration to ensure safety. A gray overcast day outdoors delivers about 10,000 lux naturally, so an early morning walk on any day is a viable alternative if you have the time and mobility.
Does light therapy work if I use it in the evening instead of the morning?
Evening light therapy produces a phase delay rather than a phase advance, pushing the circadian clock later rather than earlier. Since most depression-related circadian disruption involves a delayed clock, evening use can make things worse. Research going back to Lewy in the 1980s established that evening light is not as effective as morning light for treating SAD. The one exception is people with advanced sleep phase disorder, who wake too early and become sleepy in the early evening. For them, carefully timed evening light can help, but this should be done under clinical guidance.
How long do I need to keep using bright light therapy?
For seasonal affective disorder, the standard recommendation is to begin in autumn and continue through spring, discontinuing when natural remission occurs. Stopping mid-winter often leads to relapse within days. For non-seasonal depression, the evidence is less clear on duration, but Maruani and Geoffroy recommend continuing until depressive symptoms resolve, and maintaining treatment if symptoms return when it's stopped. There are no long-term safety concerns with ongoing use, though annual eye checkups are prudent for users over 65.
Is blue light therapy better than white light?
Blue light targets the melanopsin receptors more directly and has stronger circadian-shifting effects per lux. However, the Yale Winter Depression Research Program recommends broad-spectrum white light as the best balance of risk and benefit, because blue light carries greater risk of retinal toxicity. One study found that blue-enriched white light at just 750 lux was equally effective as standard 10,000 lux white light for SAD, suggesting the blue component matters but doesn't need to be isolated.
Will my health insurance cover a light therapy box?
Most health insurance plans, including Medicaid, do not currently cover light therapy devices. An increasing number of private insurers view light therapy as medically appropriate for patients meeting SAD diagnostic criteria, but reimbursement remains inconsistent. The out-of-pocket cost for a clinically appropriate device typically falls between $100 and $200.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.