
What Counts as Long-Term Peptide Use in 2026?
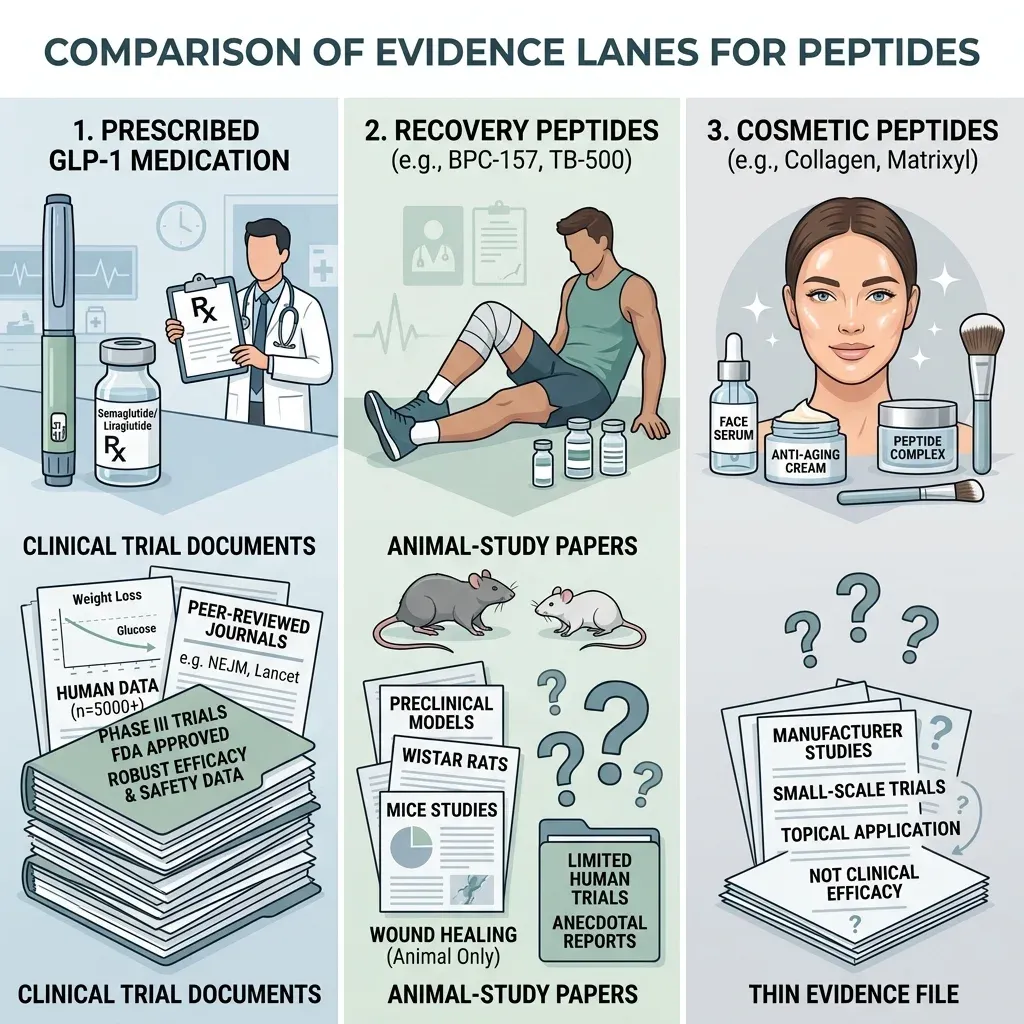
People talk about long-term peptide use as if it means one thing. It does not. A person on prescribed semaglutide, a person cycling BPC-157 for injuries, and a person using a cosmetic copper peptide are all using peptides, but the evidence behind those habits lives in different worlds.
The best long-term evidence sits with GLP-1 receptor agonists. A 2026 Drug Safety review notes that the first GLP-1 receptor agonist was approved for diabetes in 2005, and that safety data for weight-loss indications became available from 2014. That gives clinicians a real pharmacovigilance trail, even if it is still imperfect.
Even here, the ordinary research meaning of long-term is not the same as the forum meaning. One GLP-1 analysis grouped trial follow-up into windows up to 104 weeks, and the authors explained that trials beyond two years were limited enough that they treated longer follow-up together inside that endpoint. Think of this like weather data: two winters can tell you something about a coat, but they cannot prove how the fabric holds up after a decade of daily wear.
For unapproved recovery or anti-aging peptides, the gap is wider. McMaster professor Stuart Phillips wrote that a BPC-157 systematic review screened 544 papers, found 36 that met criteria, and found that 35 were rodent or cell studies, with only one human musculoskeletal study. The published human examples he listed were a 16-patient knee-pain report, a 12-woman interstitial-cystitis pilot, and a 2-person intravenous safety pilot.
For long-term peptide users, the first question is not "Does anyone online report benefits?" It is "Which peptide has multi-year human data, and which one is still mostly biology plus anecdotes?"
That distinction changes the whole article. The strongest reports from longer-term users are about persistence, stopping, rebound, monitoring, and the annoyance of staying on therapy. The weakest claims are the broad anti-aging promises, because the long-term human evidence has not caught up with the marketing.
What Five-Year Users Actually Report
The more honest phrase is not "what five-year users prove." It is "what longer-term users report." The evidence base contains scattered user narratives, forum threads, adverse-event reports, and some real-world medication studies. Those are useful signals, but they are not interchangeable.
A recent analysis discussed by MedicalXpress reviewed more than 12,000 Reddit posts about BPC-157 and related peptides after injuries or surgery. Users raised concerns about side effects, product purity, and long-term safety, including injection-site reactions, diarrhea, and emotional numbness. That is not randomized evidence. It is more like listening through the wall of a crowded waiting room: you hear patterns, but you do not know the denominator, the dose, the product quality, or what else people were taking.
Forum reports also show why users keep experimenting. Some describe injury recovery that feels faster than usual. Others describe no effect beyond irritation. Still others describe symptom flares after starting. A Reddit thread on stopping peptides asked whether new habits stuck or whether users went back to baseline, while a GLP-1 discontinuation thread centered on recovery after stopping therapy. Those narratives matter because they show the lived burden of long-term use, but the clinical rebound data below is stronger than any single thread.
| What users report | How strong the evidence is | Best interpretation |
|---|---|---|
| Better injury recovery | Weak for BPC-157 and TB-500 in humans | Possible signal, not proof |
| Injection-site reactions, diarrhea, emotional numbness | User-report analysis of more than 12,000 posts | Worth tracking as safety signals |
| Weight regain or appetite return after stopping GLP-1 therapy | Supported by clinical discontinuation studies | Expected for many users, not a moral failure |
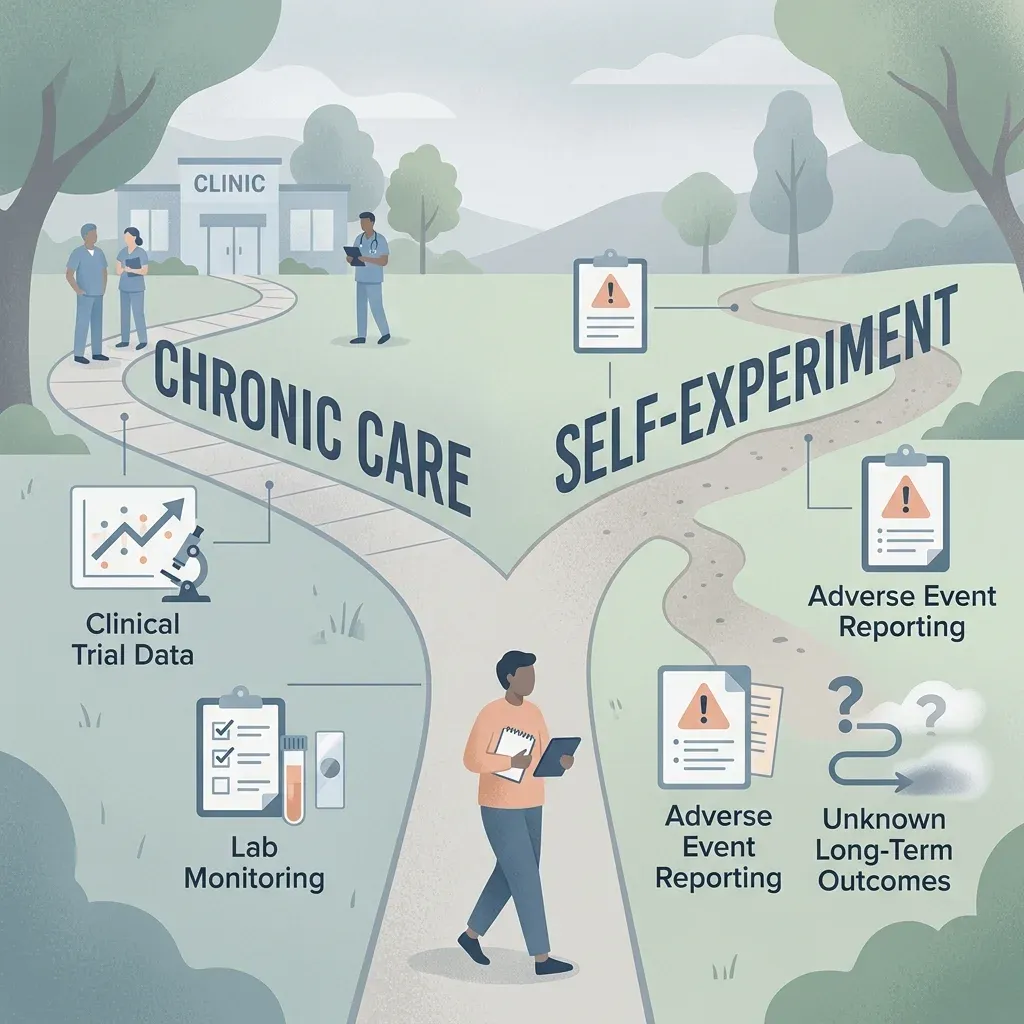
Phillips calls unauthorized peptide use high-risk, uncontrolled human self-experimentation. That sounds harsh until you look at the ingredients of a typical self-experiment: a purchased vial, a crowd-sourced dosing schedule, a subjective outcome, and no registry that follows people year after year. For the reader, the practical move is to treat long-term testimonials as leads for questions, not as a replacement for monitoring.
Persistence, Discontinuation, and the Rebound Problem
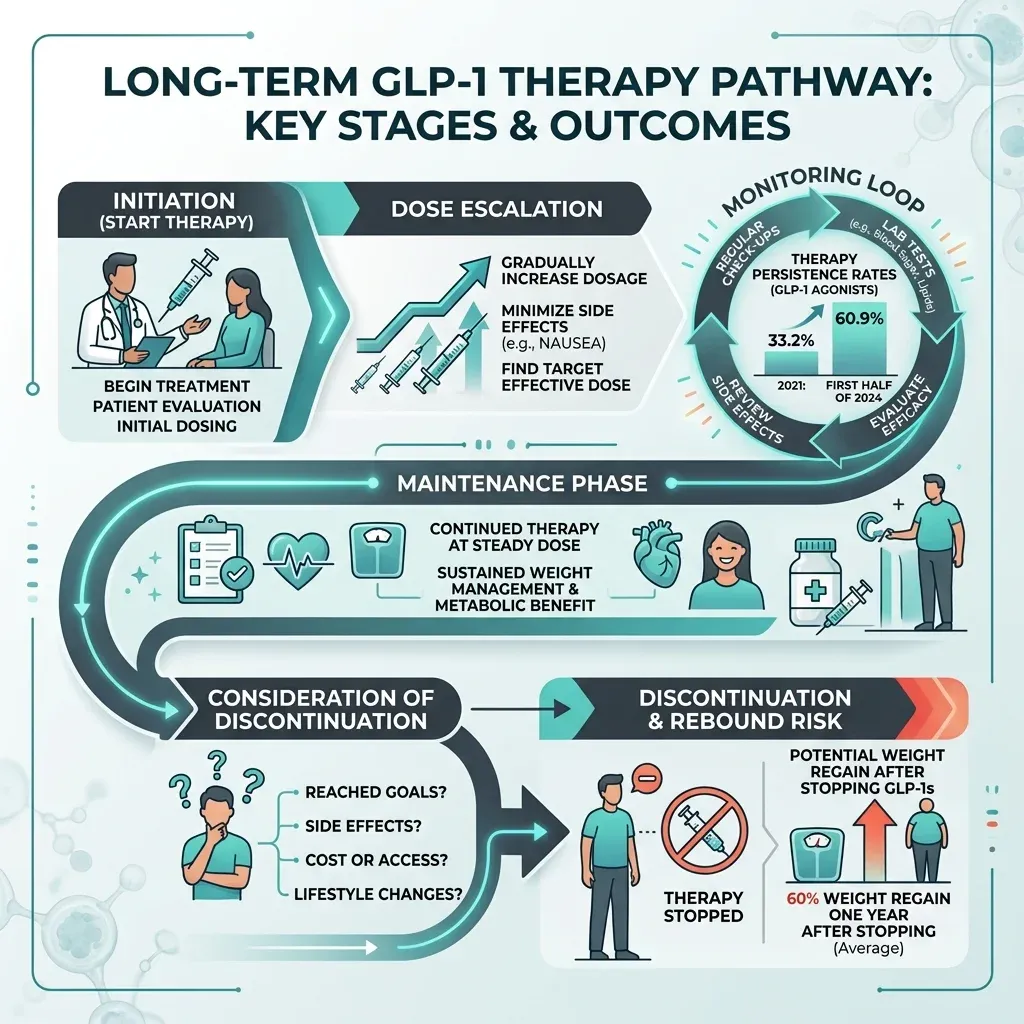
For prescribed GLP-1 drugs, the long-term story is less glamorous than the before-and-after photos. It is about whether people can stay on therapy, whether they can tolerate it, and what happens when they stop.
A Journal of Managed Care & Specialty Pharmacy cohort study followed 33,607 commercially insured adults without diabetes who started high-potency weight-loss GLP-1 therapy. One-year persistence rose from 33.2% in 2021 to 60.9% in the first half of 2024. Semaglutide persistence rose from 33.2% to 58.6% over that span, while tirzepatide persistence was 64.0% in 2023 and 64.8% in the first half of 2024.
Persistence is still fragile. In a 2025 Diabetes, Obesity and Metabolism study, Faisal I. Almohaileb, Carel W. le Roux, and Michael Crotty reported an average treatment duration of 707 +/- 425 days across 350 patients, and 174 of 350 patients were classified as having discontinued treatment. Among follow-up respondents, the reasons were ordinary and stubborn: side effects 36%, logistics 24%, cost 23%, supply shortages 11%, and dissatisfaction with weight response 7%.
The rebound data is the part long-term users talk about with the least romance. A systematic review and nonlinear meta-regression found that one year after stopping GLP-1 receptor agonists, people regained 60% of the weight lost during treatment, with regain estimated to plateau at 75.3%. A separate meta-analysis of 18 RCTs and 3,771 participants found an average 5.63 kg weight gain and a 0.25% HbA1c rise after discontinuation among individuals with obesity.
That is not a failure of willpower. It is a treatment-withdrawal pattern. If appetite and glycemic signaling are like a thermostat, GLP-1 therapy changes the setting while it is active. Remove it, and the system often drifts toward its previous temperature. The practical implication is blunt: anyone starting long-term therapy should plan the maintenance phase before the first dose, not after the last one.
Safety Signals That Matter After Years
Long-term safety is not one list of side effects. It is a sorting job. Some signals are expected and manageable. Some are rare but serious. Some belong mostly to unapproved or compounded supply chains. Mixing them together makes the whole topic either falsely terrifying or falsely casual.
For GLP-1 drugs, a JCI review says concerns that GLP-1 receptor agonists raise acute pancreatitis and pancreatic cancer risk have been dispelled by long-term trials, while thyroid-cancer uncertainty remains for susceptible individuals. The same review says sight-threatening eye complications linked to rapid glycemic reductions may be reduced by retinal screening and ophthalmologic treatment before GLP-1 initiation.
The JCI review also reports that in a systematic review, 6.5% of GLP-1RA users discontinued due to adverse events compared with 3.6% of placebo users. In another systematic review of 55 double-blind placebo-controlled RCTs, GLP-1RA therapy was associated with increased cholelithiasis risk, with RR 1.46 and 95% CI 1.09-1.97, but not with cholecystitis, cholangitis, or pancreatitis.
Compounded GLP-1 products add a different risk layer. The FDA says unapproved versions do not undergo FDA review for safety, effectiveness, and quality before marketing. FDA also reports compounded semaglutide dosing-error adverse events, some requiring hospitalization, and says that as of July 31, 2025, it had received 605 adverse-event reports for compounded semaglutide and 545 for compounded tirzepatide.
| Signal | Where it shows up | Long-term meaning |
|---|---|---|
| GI intolerance | GLP-1 trials and real-world discontinuation | Common reason users stop |
| Eye complications after rapid glycemic improvement | GLP-1 safety reviews | Screening matters before initiation |
| Immunogenicity and peptide impurities | FDA BPC-157 and injectable GHK-Cu concerns | Product quality becomes part of the safety profile |
| Bacterial endotoxin contamination | Gray-market peptide reporting | Can turn a self-experiment into an acute medical risk |
For BPC-157 and injectable GHK-Cu, FDA's language is not subtle. FDA says compounded BPC-157 may pose immunogenicity risks and that it lacks enough information to know whether it would harm humans. FDA also says injectable GHK-Cu may pose immunogenicity risks because of aggregation and peptide-related impurities, with limited human safety data.
Gray-market contamination is the most concrete fear outside the clinic. The Guardian quoted Adam Taylor warning that bacterial endotoxins in research-purpose products can trigger septic shock, and the BBC reported Taylor's warning that people using these products are becoming lab rats. The BBC story cited an analysis suggesting 8% of gray-market peptides may contain bacterial endotoxins. For someone using peptides for years, the vial becomes part of the exposure.
Monitoring Routines Long-Term Users Settle Into
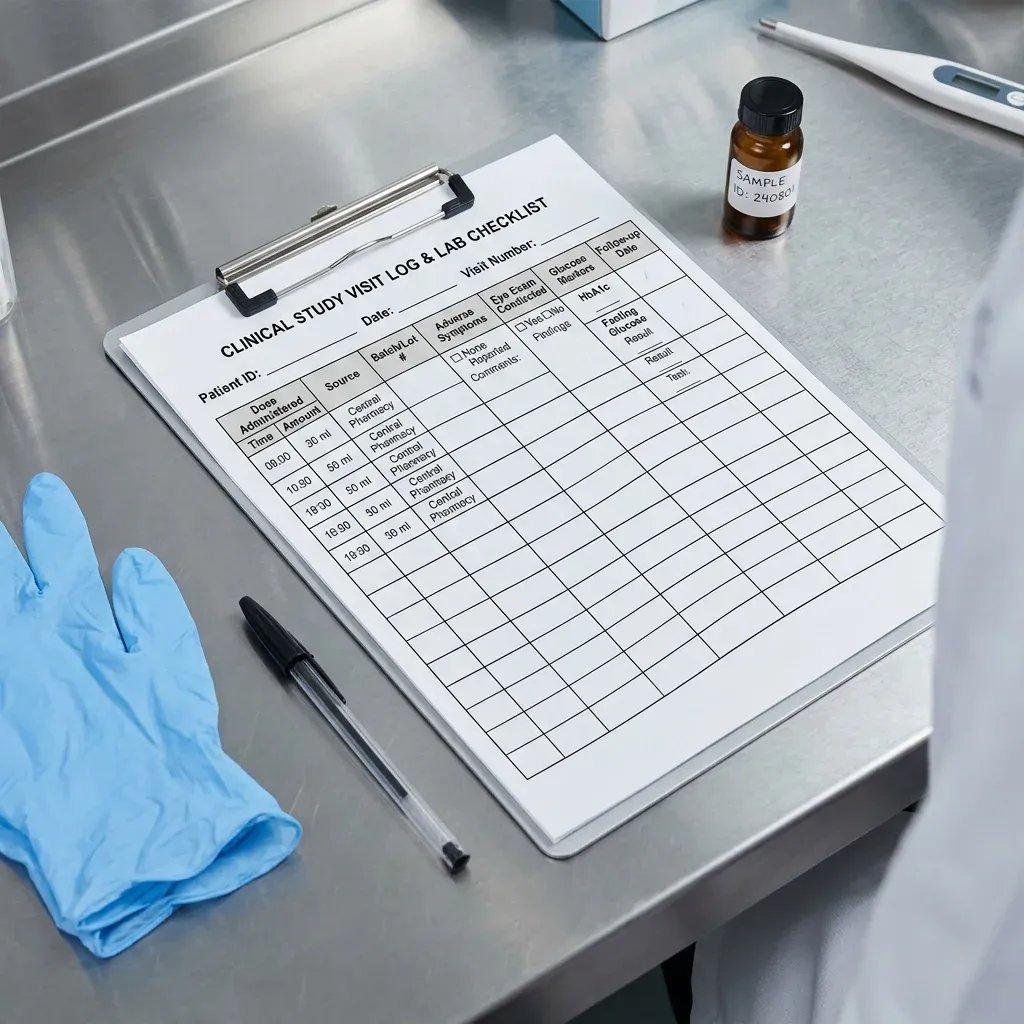
The users who seem least surprised by long-term peptide therapy are the ones who stop treating it like a temporary supplement stack. They build routines: prescriptions or sourcing records, symptom notes, dose changes, lab results, eye exams when relevant, and a clinician who knows what they are taking.
The monitoring problem is not only personal discipline. A Drug Safety review warns that private prescribing outside integrated health records can leave general practitioners unaware that patients are using GLP-1 RAs. If the clinician who sees the nausea, gallbladder pain, vision change, or anesthesia risk does not know about the drug, the safety signal can be missed.
The same review suggests several fixes: data sharing between private prescribers and GPs, EHR integration, active surveillance cohorts, and patient-experience data. That sounds bureaucratic, but in long-term use it is the difference between a smoke detector and a diary. A diary helps you remember. A smoke detector wakes somebody up.
FDA gives a smaller but practical version of the same advice for compounded semaglutide and tirzepatide: patients should talk with their health care provider or compounder about how to measure and administer the intended dose. That is basic, but basic mistakes are exactly how some dosing-error reports happen.
A useful long-term log is boring on purpose. It records the product source, dose, dose changes, symptoms, labs, procedures, and reasons for pauses. It also leaves room for "nothing happened," because no change is still data when someone is deciding whether a therapy is worth continuing. The point is not to turn patients into researchers. The point is to make sure a clinician can reconstruct the timeline if nausea becomes dehydration, an eye symptom appears after rapid glucose improvement, or a supply switch lines up with a new reaction.
| Routine | Why it matters | Evidence anchor |
|---|---|---|
| Tell every clinician what you use | Private prescriptions can be invisible in routine records | Drug Safety monitoring review |
| Document dose and titration | FDA describes dosing-error adverse events with compounded products | FDA GLP-1 concerns |
| Plan eye screening when diabetes control changes fast | Rapid glycemic improvement can surface eye risk | JCI GLP-1 safety review |
| Plan the stop or maintenance phase before starting | Weight regain after stopping is predictable for many users | GLP-1 cessation meta-regression |
VCU Health quotes Dr. Susan Wolver saying that people who succeed on GLP-1 drugs may need to stay on medication long-term, maybe for life. That is the sentence many users do not want to hear, but it is also the sentence that turns the decision from a short experiment into a chronic-care conversation.
What Is Still Unknown
The unknowns are not small footnotes. They are the center of the story for many popular peptides. Phillips writes that plausible rodent and pathway biology can create excitement before reliable clinical evidence exists. UNSW makes the same broader point: major gaps remain in whether anti-aging peptide claims stack up and whether they are safe for humans.
TB-500 is a good example. MedicalXpress explains that thymosin beta 4 biology is interesting, but TB-500 is a smaller piece of that molecule, and human recovery claims cannot be borrowed wholesale from related research. The same article warns that blood-vessel growth and cell migration also matter in scarring, abnormal tissue growth, and cancer biology, so long-term human safety must be shown rather than assumed.
FDA's July 23-24, 2026 advisory committee notice is also a clue. FDA scheduled discussion of BPC-157, KPV, TB-500, MOTs-C, DSIP/emideltide, Semax, and Epitalon bulk substances. These are not ordinary long-term maintenance drugs with settled protocols. They are still being argued over at the level of basic inclusion, safety, and appropriate compounding use.
The practical takeaway is cautious, not puritanical. Some peptide medicines are becoming chronic therapies. Some experimental peptides may eventually find specific uses. But the user report that matters most in 2026 is not "I felt better." It is "I stayed on it, I knew what I was taking, my clinician could see it, and we had a plan for what would make us stop."
Frequently Asked Questions
Is there solid evidence on five-year peptide use?
There is meaningful multi-year evidence for prescribed GLP-1 therapies, but most unapproved wellness or recovery peptides have little or no controlled human evidence extending into that range. For BPC-157, McMaster notes that one systematic review found only one human musculoskeletal study after screening 544 papers.
What do long-term GLP-1 users most often report?
The strongest pattern is persistence versus discontinuation. A JMCP study found one-year persistence rose from 33.2% in 2021 to 60.9% in the first half of 2024, while discontinuation studies show users often stop because of side effects, logistics, cost, shortages, or unsatisfying response.
What happens when people stop GLP-1 therapy?
Many regain weight. One meta-regression found that one year after stopping, people regained 60% of the weight lost during treatment, while another review found an average 5.63 kg weight gain after discontinuation among people with obesity.
Are user reports about BPC-157 and TB-500 reliable?
They are useful as safety signals, not proof. MedicalXpress reported that an analysis of more than 12,000 Reddit posts found concerns about side effects, product purity, and long-term safety, but anecdotal reports cannot establish dose, purity, causality, or long-term benefit.
What should someone discuss with a clinician before long-term peptide use?
Discuss the exact compound, source, dose, titration plan, stop plan, current diagnoses, other medicines, eye or gallbladder risk when relevant, and how adverse symptoms will be tracked. FDA specifically encourages patients using compounded semaglutide or tirzepatide to ask how to measure and administer the intended dose.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











