
The First Step Is Screening, Not a Shopping List
The wrong way to approach anti-aging peptides is to start with names: sermorelin, CJC-1295, ipamorelin, BPC-157, tesamorelin. That is how supplement shopping works. It is not how endocrine medicine works.
A more honest protocol starts with the question a good clinician would ask first: what problem are we actually trying to solve? Low energy, belly fat, weak recovery, poor sleep, low libido, and slower gym progress can overlap with sleep apnea, insulin resistance, depression, low testosterone, medication effects, thyroid disease, alcohol use, and ordinary overtraining. If you skip that step, peptides become a very expensive way to avoid a diagnosis.
Growth hormone is a useful example. Endotext notes that adult growth hormone deficiency has subtle, nonspecific features and usually requires stimulation testing to make the diagnosis, not a random single blood draw because GH secretion is episodic and modified by age, sex, and body mass index. The same chapter warns that random GH or IGF-1 values can overlap between healthy adults and adults with GH deficiency, particularly in adults older than forty so the lab number has to be interpreted in context.
A doctor-style peptide protocol begins with diagnosis, contraindications, and monitoring. If the first step is a product bundle, the protocol is already upside down.
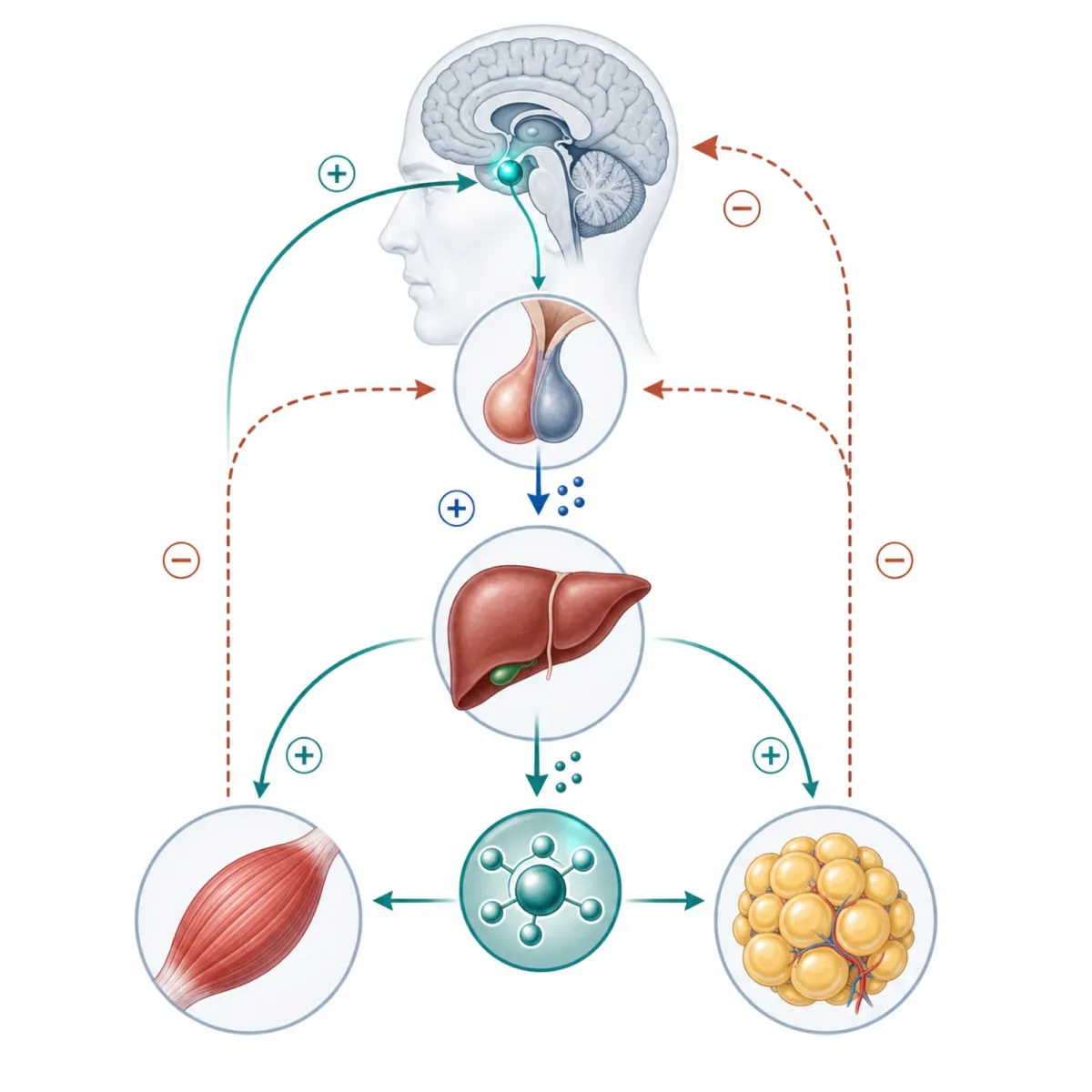
Think of the growth-hormone axis like a thermostat in a large building. A single room temperature does not tell you whether the furnace, sensor, wiring, insulation, or outside weather is the problem. In the same way, a single hormone marker rarely explains a man's whole midlife picture.
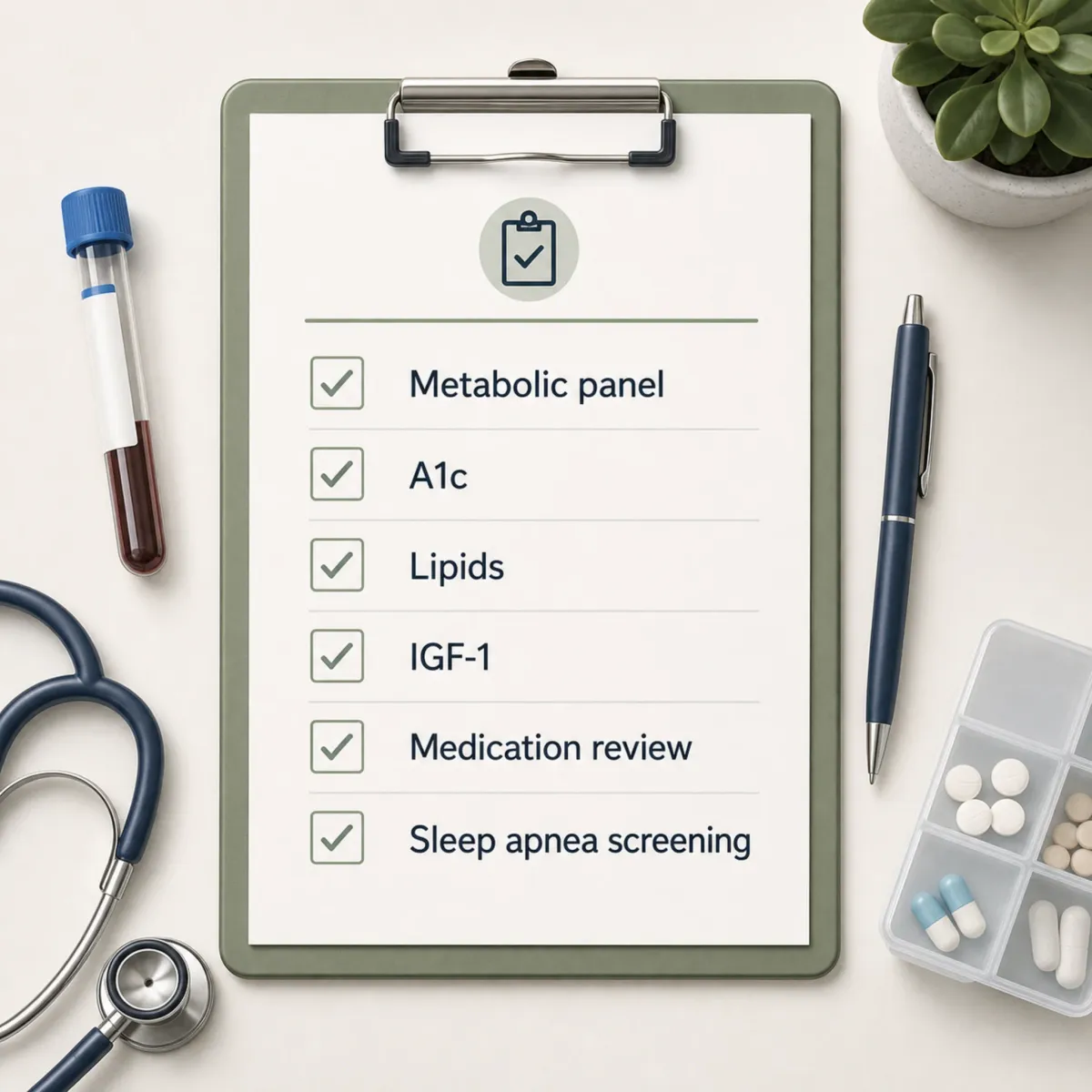
| Before peptides | Why it matters |
|---|---|
| Confirm the target problem | Fatigue, low recovery, and body composition changes are nonspecific. |
| Review medications and diagnoses | Glucose, cancer history, edema, sleep apnea, and pituitary disease change the risk discussion. |
| Run baseline labs | Tesamorelin trials tracked body composition, IGF-1, lipids, glucose, and insulin rather than symptoms alone. |
| Set a stop rule | A protocol without an exit plan quietly becomes open-ended experimentation. |
Practically, this means a man should not ask, "Which peptide should I take?" first. He should ask, "What diagnosis, risk factor, or measurable endpoint would justify taking any peptide at all?"
Which Anti-Aging Peptides Have Human Evidence?
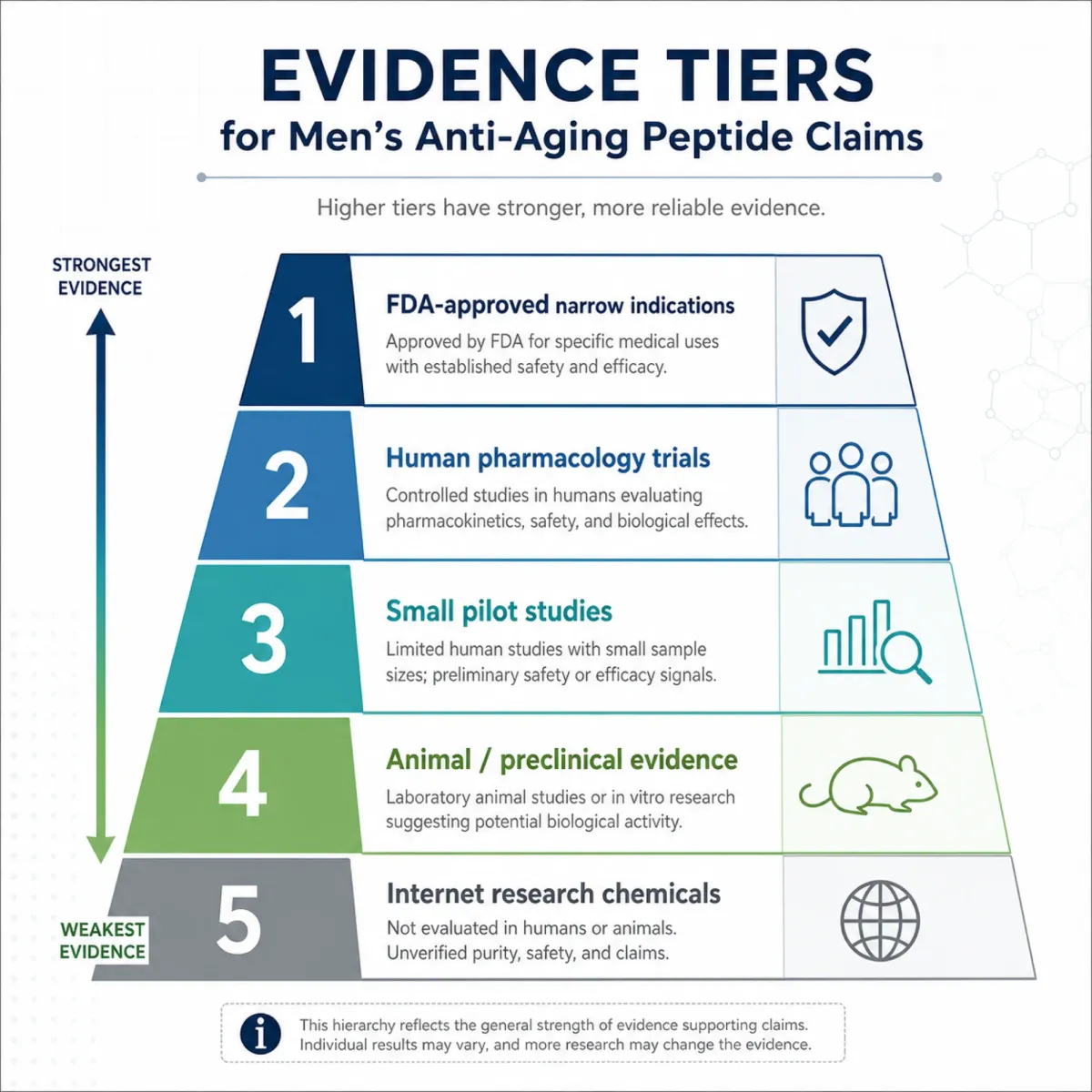
The phrase "anti-aging peptides" lumps together very different substances. Some are FDA-approved drugs for narrow indications. Some have early human pharmacology. Some have mostly animal data. Some are internet lore with a medical-sounding label.
That difference matters. A peptide with a real human trial in a specific disease population is not automatically a longevity drug for a healthy man with a busy job and a gym membership.
| Peptide or class | What human evidence actually shows | Conservative interpretation |
|---|---|---|
| Tesamorelin | In a trial of 412 HIV patients, 86% of whom were men, daily tesamorelin reduced visceral adipose tissue by 15.2% over 26 weeks. | Strongest for its approved-style metabolic niche, not a general belly-fat shortcut. |
| CJC-1295 | A healthy-adult study found one injection raised mean GH 2- to 10-fold for 6 or more days and IGF-1 1.5- to 3-fold for 9 to 11 days. | Human pharmacology exists, but that is not the same as long-term anti-aging proof. |
| BPC-157 | A sports-medicine systematic review says it has preclinical musculoskeletal evidence but lacks FDA approval and is banned in professional sports. | Do not treat animal repair data as a green light for chronic self-injection. |
| Growth hormone itself | Older GH studies showed body-composition changes, but higher-dose attempts in older adults produced frequent adverse effects including edema and impaired glucose tolerance. | More anabolic signaling is not automatically safer or younger. |
One clean way to read this evidence is to separate "signal" from "protocol." CJC-1295 clearly signals the GH axis in humans. Tesamorelin clearly changed visceral fat in a defined HIV-lipodystrophy population. Neither fact proves that a healthy man should stack multiple peptides for years.
The practical takeaway is boring, which is why it is useful: evidence should narrow the conversation, not expand it. The better the source, the more specific the indication usually becomes.
Why the Growth-Hormone Axis Gets Riskier After 40
The GH axis is the reason many peptide clinics sound persuasive. Growth hormone falls with age. Recovery feels slower. Belly fat accumulates. The pitch almost writes itself.
The physiology is real. Endotext reports that after the third decade of life, GH secretion declines about 15% per decade. It also reports that GH secretion peaks around 150 mcg/kg/day at puberty and falls to about 25 mcg/kg/day by age 55.
But a decline is not always a disease. Gray hair is a decline in pigment, not a diagnosis. The danger is assuming that every age-related drop should be pushed upward with a drug-like signal.
Endotext describes what happened when investigators tried to reproduce higher-dose GH approaches in older adults: adverse effects included fluid retention, joint pain, muscle pain, carpal tunnel syndrome, and impaired glucose tolerance. The same chapter summarizes a systematic review in healthy older adults where GH users had more soft tissue edema, arthralgias, carpal tunnel syndrome, gynecomastia, impaired fasting glucose, and diabetes onset.
That is the central tension for men over forty. The pathway you want to stimulate for muscle, recovery, and body composition is also tied to glucose handling, fluid balance, joint symptoms, and theoretical concerns around long-term growth signaling.
The practical implication is simple: if the sales pitch is "restore youthful GH," ask what the monitoring plan is for adult physiology. A younger-looking lab curve is not useful if it comes with worse glucose, swollen hands, numb fingers, or unresolved sleep apnea.
A Conservative Doctor-Style Protocol for Men Over 40
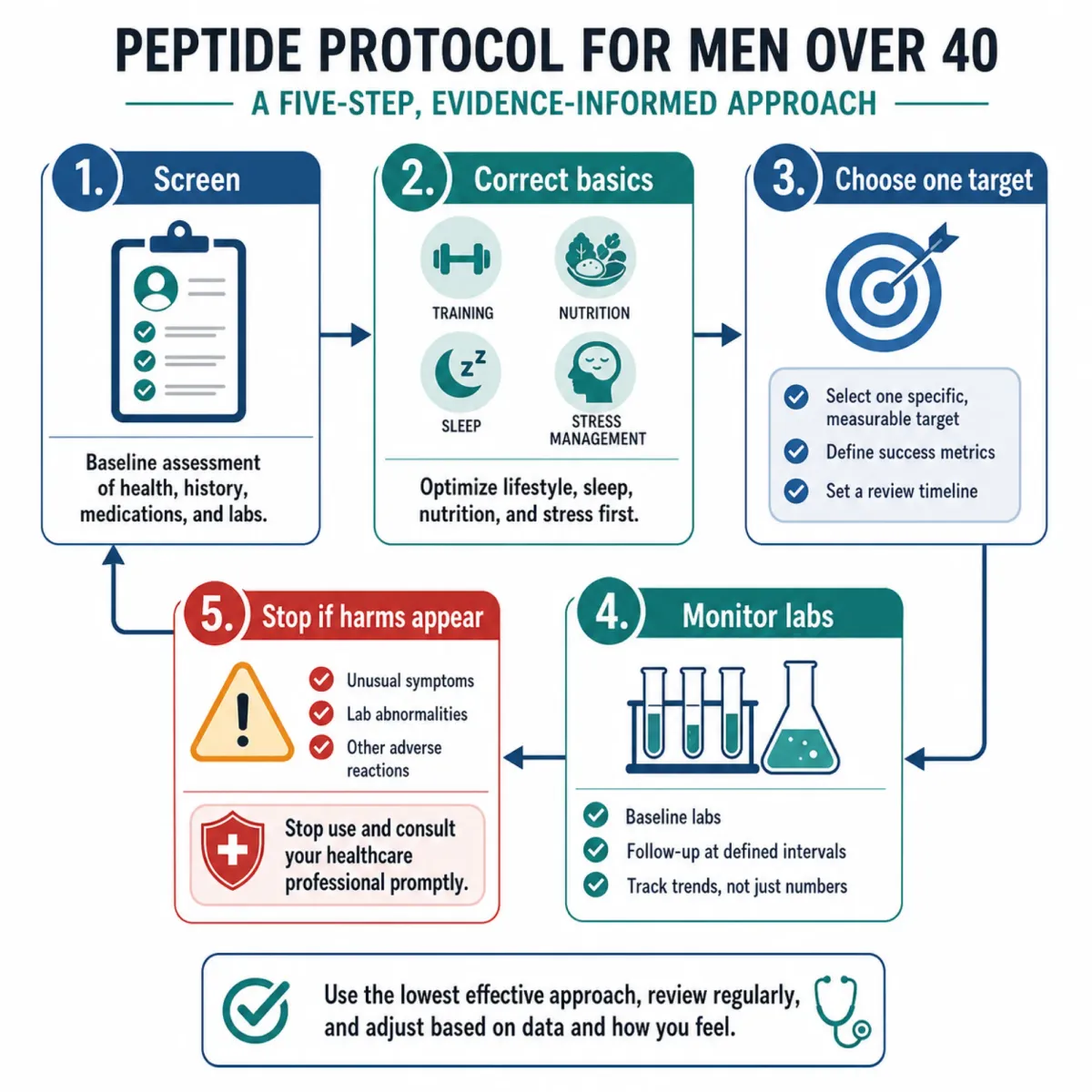
A conservative protocol is not a stack. It is a sequence of gates. Each gate either gives a clinical reason to continue or a reason to stop.
The first gate is diagnosis. For suspected adult GH deficiency, Endotext says stimulation testing should be considered only when there is clinical suspicion and the intent to treat if the diagnosis is confirmed because no single ideal test exists. The same chapter notes that BMI changes interpretation and proposes a lower glucagon stimulation cut point around 1 mcg/L in some overweight and obese patients to reduce false classification.
The second gate is basics that peptides cannot rescue. Sleep, resistance training, alcohol, protein intake, waist circumference, blood pressure, and glucose control are not wellness fluff. They are the background noise that makes hormone interpretation messy. Trying to tune peptide signaling while ignoring them is like adjusting a microphone while the fire alarm is going off.
The third gate is peptide selection. A cautious physician would not put CJC-1295, ipamorelin, BPC-157, tesamorelin, and a "longevity" peptide into one first pass. The cleaner question is whether one intervention has a plausible indication, a measurable endpoint, and a defined trial period.
| Gate | What a cautious clinician asks | What would stop the process |
|---|---|---|
| Diagnosis | Is there a real indication, not just a midlife symptom cluster? | No objective problem to follow. |
| Risk review | Any cancer history, uncontrolled glucose, edema, neuropathy, sleep apnea, or interacting medication? | A risk that makes GH-axis stimulation a poor bet. |
| Single target | Are we tracking waist, visceral fat, IGF-1, pain function, sleep, or strength? | No measurable endpoint. |
| Time limit | What changes by the reassessment date? | Open-ended use without benefit. |
For most men, this conservative sequence will point back to metabolic and recovery fundamentals before peptides. That is not a dismissal. It is risk stratification. A protocol that makes the ordinary work visible is less exciting, but it is much harder to fool.
It also keeps the conversation from becoming a status game. Men often arrive at peptide clinics after years of being told to accept fatigue as aging or to fix everything with testosterone. Peptides can look like a third door: more advanced than supplements, less loaded than hormones. The problem is that the body does not care about branding. If a peptide pushes a growth signal, changes appetite, alters water retention, or raises IGF-1, it belongs in a medical plan with a defined reason.
A cautious doctor would also avoid changing several variables at once. If sleep treatment, resistance training, nutrition, testosterone evaluation, and a peptide all begin in the same month, no one can tell what helped or what harmed. A better protocol changes the largest low-risk variable first, then reassesses. That pace feels slow, but it is how you keep cause and effect visible.
Monitoring, Lab Markers, and Stop Rules
If a peptide is strong enough to matter, it is strong enough to monitor. The best anti-aging protocol is the one with clear reasons to discontinue.
Tesamorelin trials are a useful model for monitoring because they did not rely on vibes. Investigators tracked body composition, IGF-1, lipids, glucose, and insulin during the 26-week trial. They also reported that more tesamorelin patients withdrew because of an adverse event, even though overall adverse events did not differ significantly from placebo in the main comparison.
Monitoring does not make an experimental protocol proven. It makes it less blind. For GH-axis peptides, the minimum conversation should include IGF-1, fasting glucose or A1c, lipids, blood pressure, edema, joint symptoms, numbness or tingling, sleep quality, and whether the original endpoint is improving.
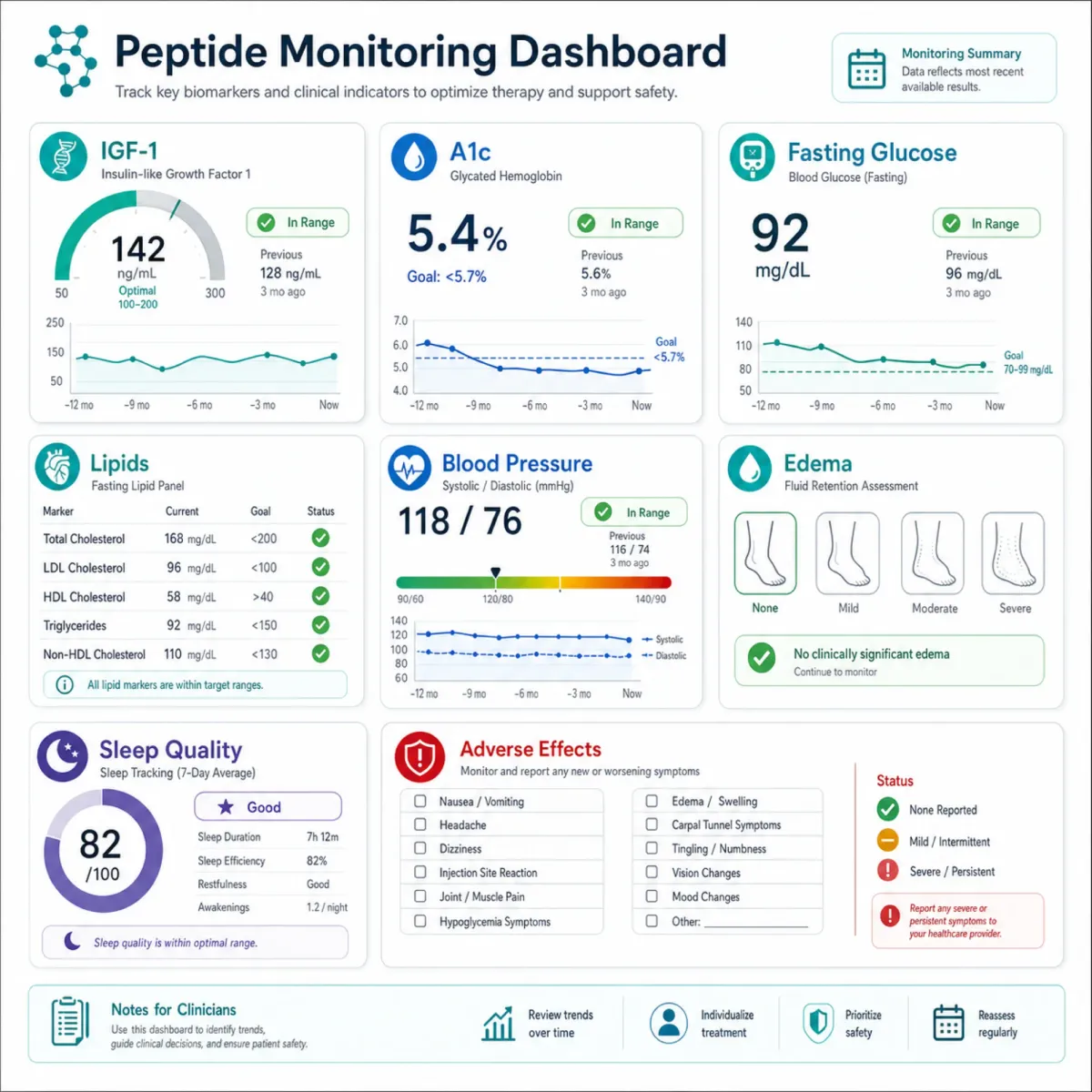
- Stop for metabolic drift: rising fasting glucose, worsening A1c, new diabetes-range results, or unexplained weight gain with swelling.
- Stop for nerve or fluid symptoms: hand numbness, carpal tunnel symptoms, persistent edema, joint pain, or rapid blood-pressure worsening.
- Stop for allergic signals: hives, spreading injection-site reactions, breathing symptoms, or systemic immune reactions.
- Stop for no benefit: if the original measurable target does not move, continuing becomes habit rather than medicine.
- Stop for legal uncertainty: if the product cannot be traced to a legitimate prescription pathway and pharmacy standard.
Even diagnostic testing has caveats. Endotext notes that macimorelin should be avoided with QT-prolonging medications and strong CYP3A4 inducers because the test has drug-interaction concerns. The insulin tolerance test historically requires adequate hypoglycemia, with blood glucose below 40 mg/dL, which is one reason alternatives exist for patients where that is inappropriate.
Practically, the monitoring visit should be scheduled before the first dose. If you cannot describe what would make you stop, you are not following a protocol. You are hoping.
Legal Status, Compounding, and Vendor Red Flags
The legal picture around peptides is not a small-print detail. It is part of the safety profile.
FDA's current 503A compounding materials say GHK-Cu was removed from category one after nominations were withdrawn, while FDA plans to consult the Pharmacy Compounding Advisory Committee before the end of February 2027. The same FDA document says BPC-157 was removed from category two after nominations were withdrawn, with PCAC review scheduled for July 23, 2026.
The meeting agenda itself lists BPC-157, KPV, TB-500, MOTs-C, DSIP, Semax, and Epitalon-related bulk substances for discussion on July 23-24, 2026. That is not the same as approval. It means regulators are reviewing whether these bulk substances belong in a compounding pathway.
| Red flag | Why it matters |
|---|---|
| "Research use only" sold for personal injection | The label itself is telling you it is not a patient-ready drug. |
| No prescription or medical record | No one owns the contraindication check, dose decision, or adverse-event follow-up. |
| Stack sold as one-size-fits-all | The risks of combining multiple growth and repair signals are not well defined. |
| Claims of guaranteed fat loss, youth, or injury repair | The strongest human evidence is narrower than the marketing. |
This is where men over forty need to be especially skeptical. A product can feel "medical" because it is injectable, refrigerated, and described with acronyms. That does not make it approved, sterile, indicated, or appropriate.
The other red flag is certainty. A legitimate discussion sounds conditional: if your labs show this, if your risk profile allows that, if the pharmacy pathway is legal, if the endpoint improves. A sales page sounds frictionless. It promises recovery, libido, fat loss, younger skin, and better sleep as if one pathway can be safely turned up without tradeoffs.
Regulation can feel frustrating when someone is desperate for relief, but it also creates accountability. When a substance moves in and out of compounding categories, or sits on a committee agenda, that should make a patient more careful, not more willing to buy from a gray-market vendor before access changes again.
Questions to Ask Before You Consider Peptides
The best questions are not hostile. They are clarifying. A legitimate clinician should be able to answer them without treating you as difficult.
- What exact diagnosis or measurable problem are we treating?
- Is this peptide FDA-approved for my indication, or are we discussing investigational or off-label use?
- What are my contraindications?
- What baseline labs will we check, and when will we repeat them?
- What side effect would make us stop immediately?
- What result would make us stop because it did not work?
- Where exactly is the product coming from?
A reasonable protocol should distinguish confirmed GH deficiency from non-approved use for aging or sporting enhancement because Endotext explicitly separates appropriate GH replacement from non-approved conditions. It should also include follow-up for glucose, insulin or A1c, lipids, IGF-1, symptoms, and adverse events, because those are the kinds of markers tracked in serious GH-axis studies rather than after-the-fact testimonials.

The honest answer may be, "not yet." That is a perfectly good medical outcome. It means the risks, legal status, or evidence did not clear the bar today.
Frequently Asked Questions
Are anti-aging peptides recommended for all men over 40?
No. The evidence supports narrow medical uses and selected human pharmacology findings, not blanket anti-aging use. A safer starting point is screening, risk review, and fixing sleep, metabolic, and recovery basics before considering any peptide.
Is sermorelin or CJC-1295 safer than HGH?
They are different ways of stimulating the GH axis, but "different" does not mean risk-free. CJC-1295 has human data showing prolonged GH and IGF-1 stimulation after a single injection, so it deserves the same caution around glucose, edema, IGF-1, and long-term uncertainty.
What labs should a doctor check before GH-axis peptides?
The discussion commonly includes IGF-1, fasting glucose or A1c, lipids, blood pressure, medication review, sleep apnea risk, and whether formal GH stimulation testing is clinically justified. Random GH or IGF-1 alone is usually not enough to diagnose adult GH deficiency because values overlap in adults.
Are BPC-157 and similar recovery peptides legal?
Legal status depends on the substance, route, indication, and compounding pathway. FDA materials currently describe BPC-157-related bulk substances as under PCAC review rather than broadly approved for routine anti-aging use on the July 2026 agenda.
When should someone stop peptide therapy?
Stop and contact a clinician for allergic symptoms, spreading injection reactions, edema, numbness, worsening glucose, blood-pressure changes, unexplained pain, or no measurable benefit by the planned reassessment date. A protocol without stop rules is not conservative care.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











