
What Founder Peptide Stacks Get Right and Wrong
The founder version of longevity is rarely subtle. It treats the body like a product roadmap: measure everything, ship interventions, iterate fast. Peptide stacks fit that mindset because peptides sound like precise biological commands rather than blunt drugs.
That part is not fantasy. Peptides are short amino-acid chains that act as cellular messengers, and medicine already uses peptide-based therapies, including insulin and GLP-1 drugs according to KalingaTV's report on the Silicon Valley peptide trend. Think of them as small text messages sent between tissues. The problem is that not every message is safe to broadcast through the whole body.
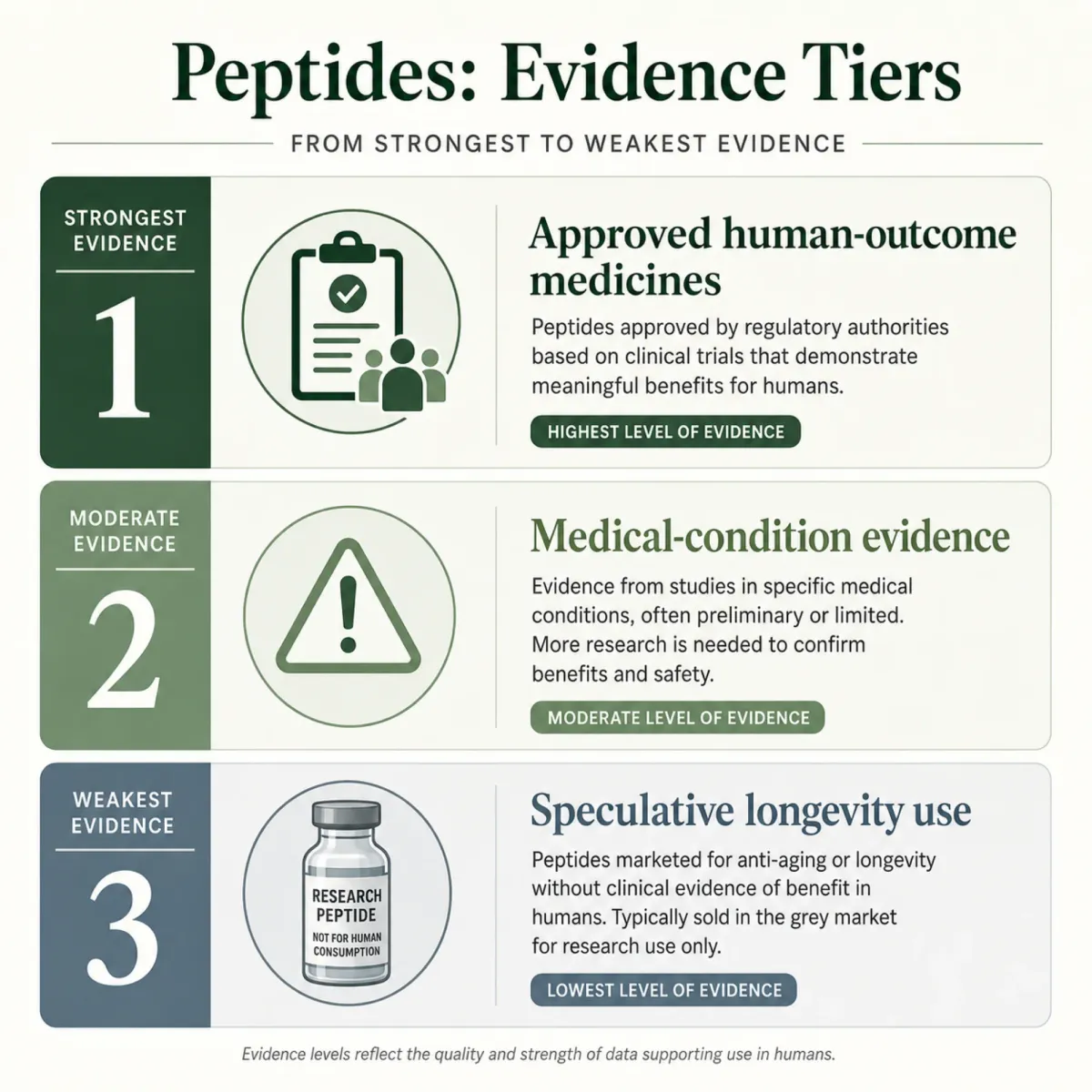
The real split is between approved peptide medicines with human outcome data and grey-market injectable compounds sold with thin evidence. The Guardian reports that peptides such as BPC-157, GHK-Cu, and TB-500 have become popular among biohackers while remaining unapproved, experimental, and short on reliable safety data in its 2026 investigation. McGill's Office for Science and Society makes the same basic point: unregulated peptide products may not contain the advertised compound, and contamination is a real concern in its BPC-157 review.
The useful question is not "Which peptide is trendy?" It is "Which claim has human evidence, a regulated product, and a risk profile I can actually verify?"
Stacking compounds raises the stakes. If someone combines a metabolic drug, a growth-hormone secretagogue, a repair peptide, an immune peptide, and a telomere peptide, any benefit or side effect becomes harder to attribute. That is like changing several variables in a software release and then trying to debug one crash report.
The practical takeaway is blunt: the peptide category contains both serious medicines and speculative biohacks. Treating them as a single bucket is how smart people end up making very expensive guesses.
1. GLP-1 Drugs: The Metabolic Bet With Real Human Data
If a founder stack has one peptide category that deserves a serious evidence conversation, it is the GLP-1 family. Semaglutide and tirzepatide are not fringe longevity hacks. They are regulated drugs studied in large human populations.
A Nature Medicine real-world study examined U.S. insurance-program patients from 2018 to 2025 and compared cardiovascular outcomes for semaglutide and tirzepatide in people with type 2 diabetes and elevated cardiovascular risk in Nature Medicine. In expanded populations, semaglutide versus sitagliptin produced a myocardial-infarction-or-stroke hazard ratio of 0.82, while tirzepatide versus dulaglutide produced a composite endpoint hazard ratio of 0.87 when mortality was included in the same study. The head-to-head tirzepatide-versus-semaglutide comparison landed at 1.06, which the authors interpreted as broadly comparable cardiovascular benefit in clinical practice in that analysis.
| GLP-1/GIP comparison | Outcome signal | Why founders care |
|---|---|---|
| Semaglutide vs. sitagliptin | HR 0.82 for myocardial infarction or stroke in Nature Medicine | Cardiometabolic risk is a major aging bottleneck |
| Tirzepatide vs. dulaglutide | HR 0.87 for composite outcome including mortality in Nature Medicine | Dual incretin signaling may offer strong metabolic leverage |
| Tirzepatide vs. semaglutide | HR 1.06 in head-to-head comparison in Nature Medicine | The question shifts from hype to patient fit |
A ScienceDirect review by Dr. James O'Keefe and colleagues goes further, framing tirzepatide and semaglutide as "anti-consumption" agents that may reduce risks tied to obesity, cardiometabolic disease, sleep apnea, kidney disease, liver disease, osteoarthritis, and premature mortality in Progress in Cardiovascular Diseases. That does not make them magic longevity drugs for healthy, lean adults. It does mean they have a stronger human-evidence base than most compounds sold as anti-aging peptides.
The mechanism is not just appetite suppression. GLP-1 drugs change metabolic traffic: hunger signals, insulin response, inflammation, and cardiovascular strain all move through connected lanes. If the body is a city, GLP-1 therapy is not a new sports car; it is a traffic-control system that can reduce jams in people whose roads are already overloaded.
The practical point is simple. For someone with obesity, diabetes, or high cardiometabolic risk, GLP-1 therapy belongs in a physician-led medical conversation. For a healthy founder using it because "longevity Twitter" said so, the evidence is much less direct.
2. Growth-Hormone Secretagogues: Recovery Promise, Aging Tradeoffs
Growth-hormone secretagogues appeal to founders because they promise recovery without admitting fatigue. Sermorelin, CJC-1295, and ipamorelin are marketed as ways to nudge the pituitary toward more growth-hormone signaling instead of injecting growth hormone directly.
Sermorelin is a synthetic form of growth hormone-releasing hormone used to raise human growth hormone according to Healthline's medical review. Healthline also notes that sermorelin is not currently available in the U.S. as an FDA-approved medication, though compounded versions may be obtained in the same review.
The tradeoff is that growth signaling is not a free upgrade. Growth hormone raises IGF-1, can interfere with insulin action, and can raise blood sugar according to a peptide-therapy clinical brochure captured in the research corpus. The same source lists impaired glucose tolerance and insulin resistance as concerns in the growth-hormone context in that document.
That is the part marketing often sands down. In a younger injured athlete, a growth-and-recovery signal may sound attractive. In an aging adult trying to avoid cancer, insulin resistance, and organ strain, more growth is not automatically better. A thermostat analogy helps: turning heat higher is useful if the room is cold, but reckless if the wiring is already overloaded.
| Stack logic | Evidence concern | Reader takeaway |
|---|---|---|
| More growth hormone for recovery | IGF-1 and glucose effects matter | Use labs and diagnosis, not vibes |
| Compounded sermorelin access | Not currently FDA-approved as a marketed U.S. medication | Verify prescriber, pharmacy, and indication |
| CJC/ipamorelin clinic protocols | Promotion runs ahead of aging-outcome trials | Do not equate hormone movement with longevity |
The practical takeaway: growth-hormone secretagogues are not casual wellness tools. If they are on the table, the conversation should include glucose, IGF-1, sleep apnea, cancer history, edema, joint symptoms, and the reason for treatment.
3. BPC-157 and TB-500: Repair Peptides With a Human-Evidence Gap
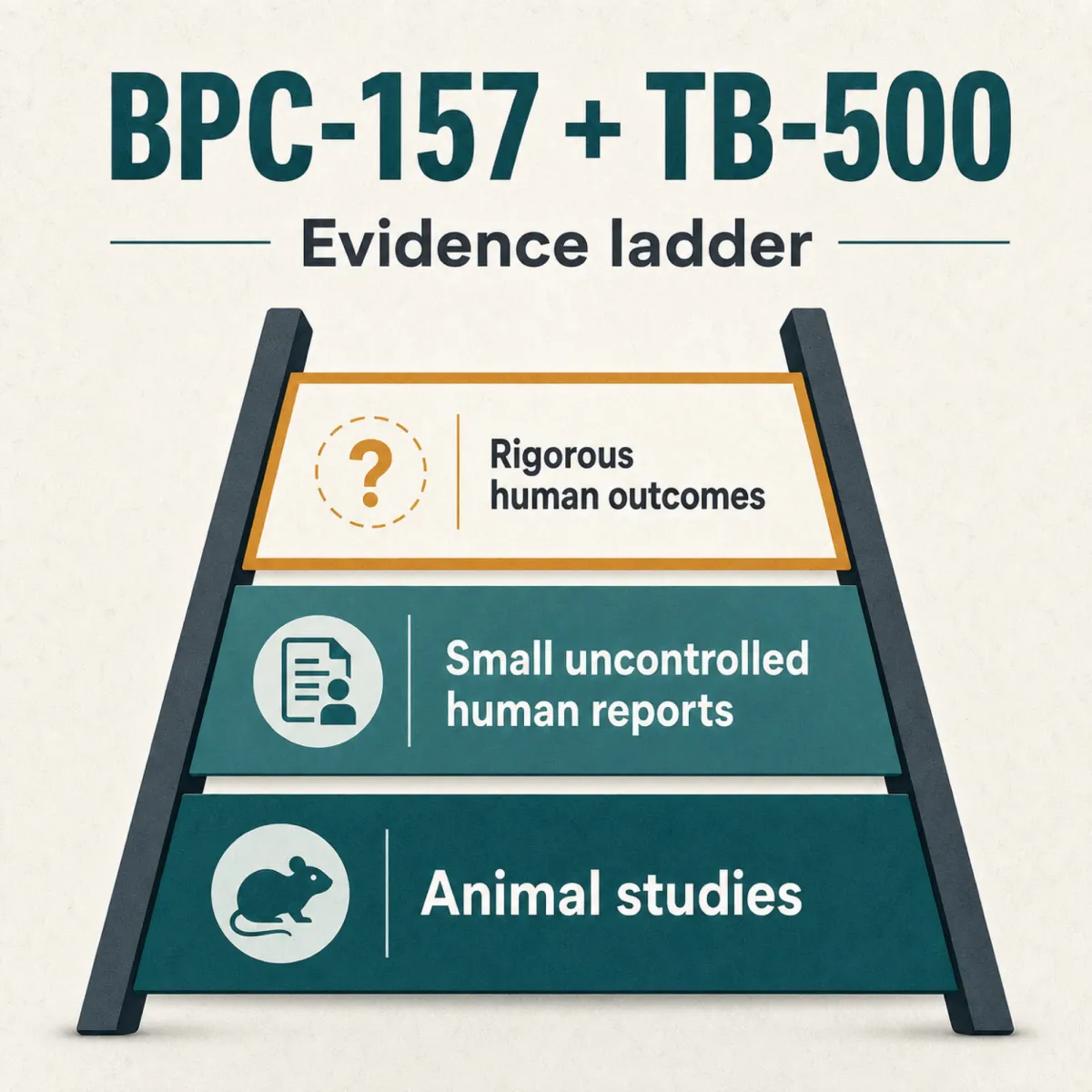
BPC-157 and TB-500 are the repair peptides that make founders feel like biology has an undo button. The pair is often marketed as the Wolverine stack, named after the fictional character's regenerative powers as The Guardian reported.
The evidence is nowhere near that cinematic. STAT/Undark reported that Dr. Flynn McGuire at University of Utah Health found almost all existing BPC-157 data comes from one Croatian research group, with very little evidence on how the drug works in humans in its BPC-157 investigation. McGill's Office for Science and Society reports that only three publications had administered BPC-157 to humans, including small uncontrolled pain studies in its review.
That is a giant gap for a compound people inject into themselves. McGill also states that BPC-157 is not FDA-approved and is listed as prohibited by the Department of Defense and WADA in the same review. The FDA's July 23-24, 2026 Pharmacy Compounding Advisory Committee meeting page confirms that peptide compounding remains an active regulatory topic on FDA.gov.
The danger is not just that BPC-157 might fail. It is that tissue-repair signaling can overlap with unwanted growth signaling. The Guardian cites experts warning that because some peptides affect tissue growth, they could theoretically accelerate an early cancer someone does not yet know about in its safety discussion. McGill adds that related trefoil peptides have been detected in tumors and may play roles in metastasis models in its mechanistic caution.
The practical takeaway is not "never study repair peptides." It is: do not confuse a plausible healing signal with a proven human therapy, especially when the product source is unregulated.
4. Thymosin Alpha-1: The Immune-Aging Candidate
Thymosin alpha-1 is the immune peptide in the stack conversation. The longevity pitch is easy to understand: the thymus helps train immune cells, immune function declines with age, so a thymic peptide sounds like a way to keep the body's security team sharp.
There is real medical research here, but it is mostly disease-context research, not preventive longevity proof. A Frontiers systematic review and meta-analysis on severe acute pancreatitis included five randomized controlled trials and 706 patients in Frontiers in Immunology. The authors reported that thymosin alpha-1 increased CD4+ T-cell percentages with a mean difference of 4.53 and P<0.00001 in that meta-analysis. The same paper notes that severe acute pancreatitis carries a mortality rate over 30% in its background section.
That makes thymosin alpha-1 more interesting than a random influencer vial. It also shows the boundary. Helping immune balance in severe illness is not the same as proving a healthy founder will live past 100 by cycling thymosin alpha-1. The immune system is not a volume knob; it is closer to an orchestra. Louder strings do not help if the percussion is already drowning out the room.
For readers, the honest use case is medical-context discussion: recurrent infections, immune compromise, or specialist-guided treatment questions. The longevity use case remains a hypothesis until healthier aging adults are studied directly.
5. Epitalon: The Telomere Claim That Needs Context
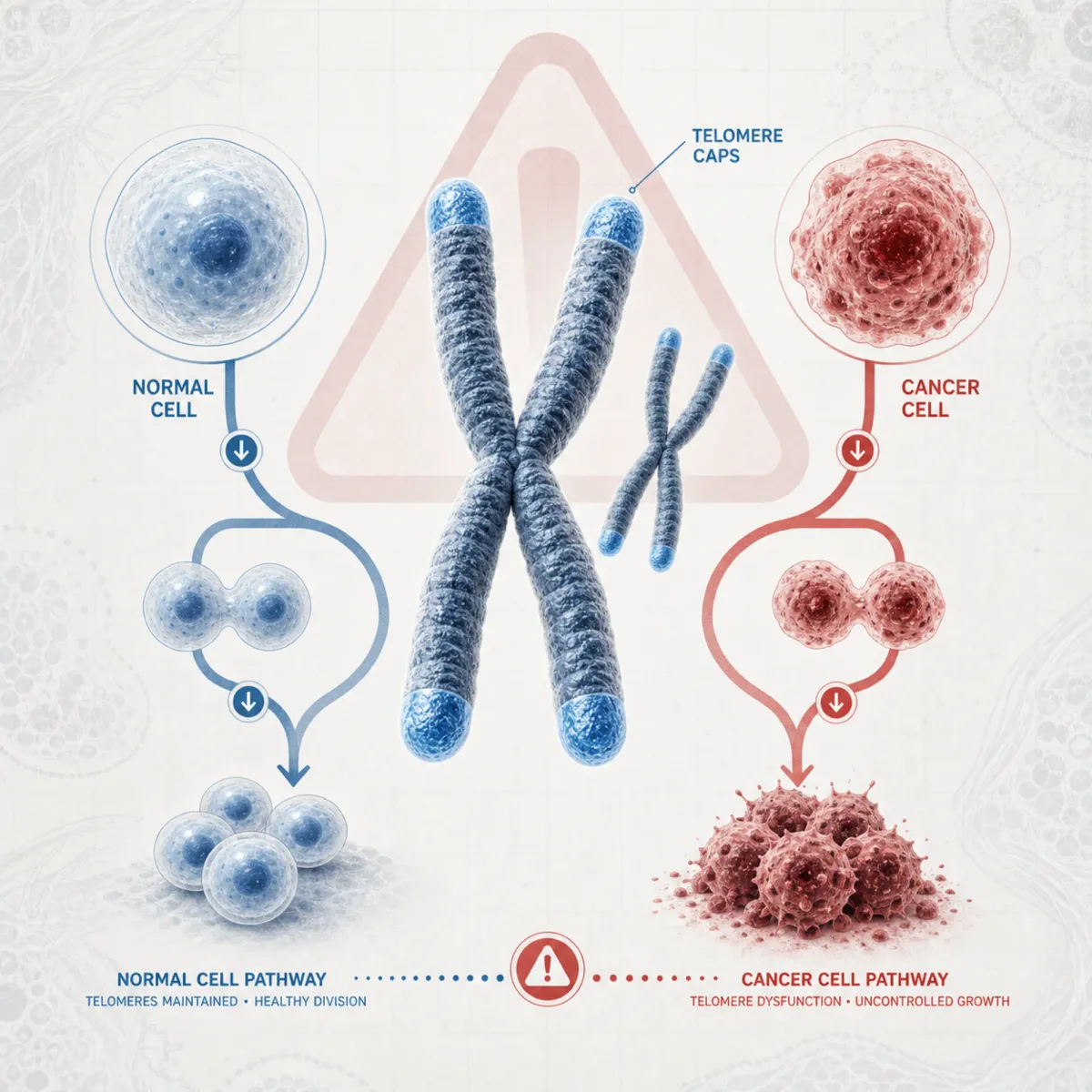
Epitalon is the stack's most seductive molecule because it lets marketers say "telomeres." Telomeres are protective chromosome caps, like plastic tips on shoelaces. Telomerase can help maintain them, which is why the idea of a telomere peptide travels so fast.
A PMC cell-line paper describes epitalon as a naturally occurring tetrapeptide known for anti-aging effects on mammalian cells in the article abstract. The same paper reports dose-dependent telomere extension in normal cells through TERT mRNA expression and telomerase activity in its results summary. It also found significant telomere extension in cancer cells through alternative lengthening of telomeres activity in that same mechanistic report.
That last line is the sober part. A telomere-lengthening signal in a dish is biologically interesting, but cancer biology is also wrapped around telomere maintenance. This is not a supplement-like claim where "more" automatically sounds good.
An MDPI overview identifies epitalon as the four-amino-acid peptide Ala-Glu-Asp-Gly and says the mechanisms remain uncertain despite extensive in vitro, in vivo, and in silico study in its review. NotebookLM's synthesis from the fetched corpus also found animal-study claims that epitalon increased maximum lifespan in one mouse strain by 12.3% and the lifespan of the last 10% of survivors by 13.3% based on the MDPI review's lifespan discussion.
| Peptide | Most defensible claim | Biggest caveat |
|---|---|---|
| GLP-1/GIP drugs | Human cardiometabolic outcome evidence | Longevity use in healthy lean adults is unproven |
| Growth-hormone secretagogues | Can move growth-hormone signaling | Growth signaling has glucose and IGF-1 tradeoffs |
| BPC-157/TB-500 | Popular repair narrative | Human evidence is thin and regulatory concerns are real |
| Thymosin alpha-1 | Disease-context immune modulation data | Preventive longevity use remains unproven |
| Epitalon | Telomere and animal-longevity signals | Human longevity benefit is not established |
The practical takeaway: epitalon belongs in the "interesting but not settled" bucket. A founder may be comfortable with uncertainty. Your cells do not care how high someone's risk tolerance is.
How to Evaluate a Longevity Stack Without Becoming the Experiment
Bryan Johnson's public Don't Die protocol includes a topical scalp serum with eight biomimetic peptides, including EGF, thymosin-beta-4, VEGF, and copper tripeptide-1 on his protocol page. That detail matters because the most visible longevity protocols often mix regulated habits, consumer products, and speculative biology under one polished dashboard.
The bigger market is much messier. The Guardian reported that U.S. customs data showed peptide and hormone-compound imports from China doubled year over year to $328 million in the first three quarters of 2025 in its reporting on peptide imports. That number does not prove every vial is dangerous, but it shows how quickly demand can outrun oversight.
Use a practical filter: ask whether the peptide has human outcomes for your actual condition, whether the product is regulated and prescribed for a clear indication, and what failure would look like: hypoglycemia, infection, immune reaction, insulin resistance, edema, tumor acceleration, or simply wasted money.
For most readers, the safest longevity stack still looks boring: sleep, resistance training, protein adequacy, blood pressure control, lipid control, glucose control, alcohol moderation, and evidence-based treatment when a real diagnosis exists. Peptides may eventually become part of that picture. The founder mistake is acting as if the future evidence has already arrived.

Frequently Asked Questions
Are tech-founder peptide stacks proven to extend lifespan?
No. GLP-1 drugs have meaningful human cardiometabolic data, but most repair, immune, growth-hormone, and telomere peptides used in longevity stacks do not have direct evidence showing that healthy adults live longer.
Which peptide in the stack has the strongest human evidence?
GLP-1/GIP drugs such as semaglutide and tirzepatide have the strongest human outcome evidence in this research package, especially for people with obesity, diabetes, or cardiovascular risk according to Nature Medicine.
Is BPC-157 safe because it is based on a naturally occurring compound?
No. McGill reports that BPC-157 is not FDA-approved, has very limited human evidence, and may be sold through unregulated sources that do not guarantee purity in its review.
Does epitalon lengthen telomeres in humans?
The strongest fetched source here showed telomere effects in cell lines, not a proven human lifespan effect in the PMC paper. Human longevity claims remain much less certain.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











