A drug from the 1960s is changing how we treat depression
Ketamine was synthesized in 1962 by chemist Calvin Stevens as a safer alternative to PCP. The FDA approved it as an anesthetic in 1970, and it became a fixture in settings from Vietnam War field hospitals to veterinary clinics. Its psychiatric potential went unnoticed for decades.
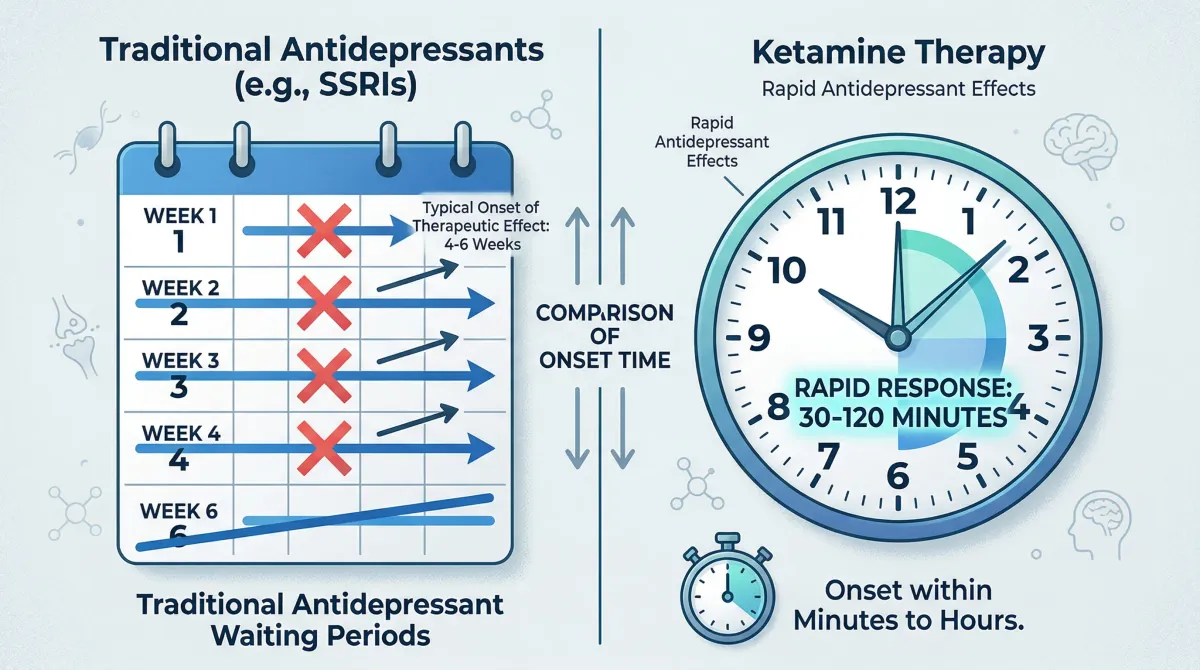
That changed in 2000, when Yale psychiatrist John Krystal published a study showing that a single low dose of ketamine could lift severe depression within hours. In a field where the standard advice was "wait four to six weeks and see," that timeline was hard to believe.
Depression affects roughly 300 million people worldwide. About 31% of patients with major depressive disorder don't respond to at least two rounds of antidepressants, which clinicians call treatment-resistant depression (TRD). These patients cycle through medications for months or years, often losing jobs, relationships, and hope in the process. The economics are grim: MDD costs the United States an estimated $326.2 billion annually, with TRD cases running 53-91% higher costs than non-resistant depression.
Ketamine therapy targets this population. A meta-analysis of 79 real-world studies covering 2,665 patients found a 45% response rate and 30% remission rate for treatment-resistant cases. Yale Medicine psychiatrist Gerard Sanacora puts the figure at 40 to 60 percent of patients. For a population that has already failed multiple treatments, those numbers matter.
Prescriptions have followed the research. Ketamine prescriptions have increased 5.5-fold since 2017, and hundreds to thousands of independent clinics have opened across the country, almost all since 2019. The growth has outpaced regulation.
How ketamine rewires the depressed brain
Traditional antidepressants (SSRIs like Prozac, SNRIs like Effexor) work by adjusting serotonin or norepinephrine levels. They slowly turn up the volume on specific neurotransmitter channels. Ketamine operates on the brain's glutamate system, the main excitatory neurotransmitter network, and helps the brain build new wiring.
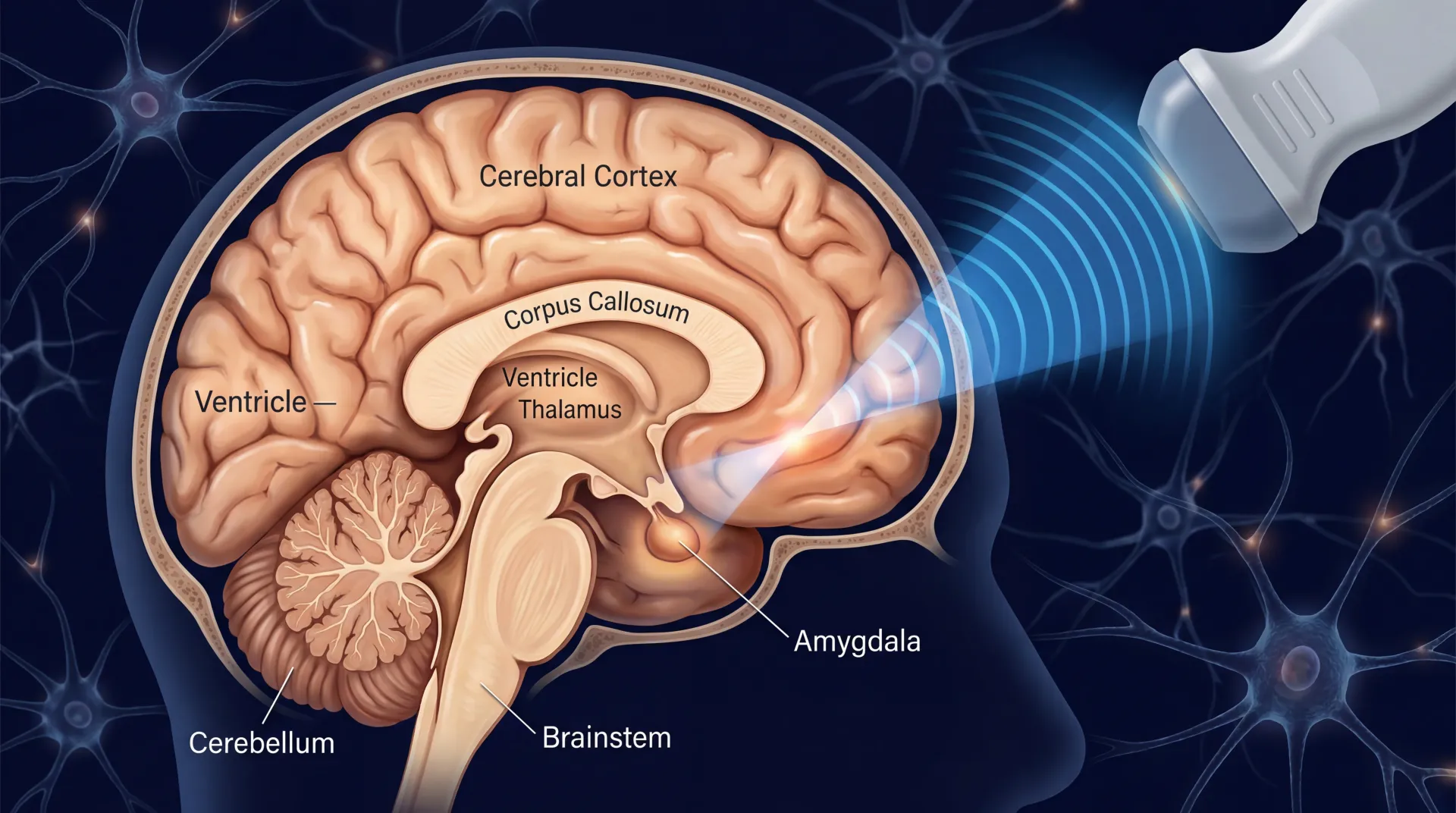
Here's what happens at a molecular level: ketamine blocks NMDA receptors, which triggers a cascade of downstream effects. AMPA receptor activation increases, boosting release of brain-derived neurotrophic factor (BDNF). BDNF activates the mTORC1 pathway, and the result is synaptogenesis — the brain growing new synaptic connections between neurons. Yale neuroscientist Ronald Duman showed that these new connections form in brain regions damaged by chronic stress and depression, restoring communication networks that had deteriorated.
If traditional antidepressants adjust signal strength, ketamine repairs damaged cables. That explains the different timescale. A meta-analysis of 9 randomized controlled trials confirmed that ketamine's effects begin about 40 minutes after infusion, peak around 24 hours, and last 3-7 days. Ketamine loses its advantage over placebo after 10-12 days, which is why patients need repeated treatments.
There's a complication worth mentioning. In 2023, Stanford Medicine researchers led by Boris Heifets ran a clever study: they gave 40 patients with moderate-to-severe depression either ketamine or placebo while under general anesthesia for routine surgery, so nobody could tell which they received. Both groups saw roughly a 50% drop in depression scores. "I was very surprised," Heifets said, "especially having talked to some of those patients who said 'My life is changed' — but they were in the placebo group."
That doesn't mean ketamine is "just a placebo," as Heifets himself stressed. The brain's opioid receptors, which process both hope and pain, may play a role in both the placebo response and ketamine's mechanism. Expectation and pharmacology probably work together, though researchers haven't fully sorted out how much each contributes. For patients weighing treatment, this is somewhat reassuring: the therapeutic context — a safe clinical setting, the sense of agency in trying something new — may amplify ketamine's biochemical effects rather than replace them.
IV ketamine vs. esketamine: two paths, different trade-offs
Two forms of ketamine are used clinically. They aren't interchangeable.
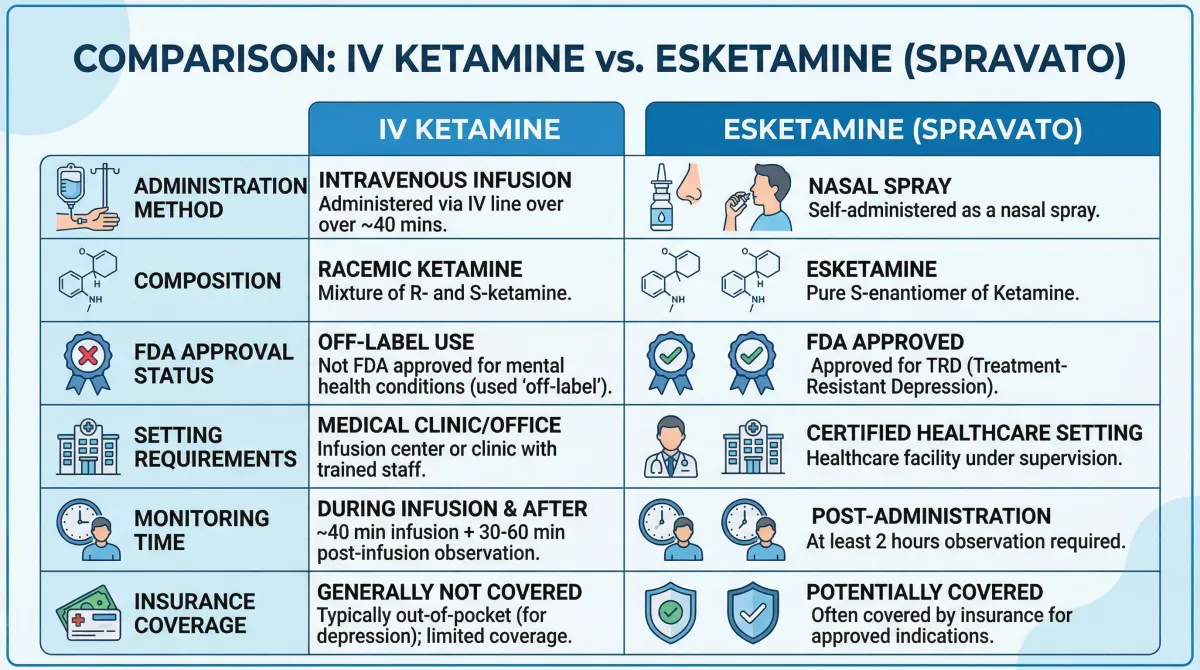
IV racemic ketamine contains both the R and S mirror-image molecules. It's given as an intravenous infusion, typically at 0.5 mg/kg over 40 minutes. The FDA approved ketamine as an anesthetic, not for depression, so every psychiatric use is off-label. Clinics can offer it without the regulatory guardrails that come with FDA-approved indications.
Intranasal esketamine (Spravato) contains only the S-enantiomer and was FDA-approved in 2019 for treatment-resistant depression and in 2020 for major depression with acute suicidal ideation. Because of safety concerns, esketamine operates under a Risk Evaluation and Mitigation Strategy (REMS) that requires administration in certified healthcare settings with a minimum two-hour monitoring period after each dose.
Head-to-head data increasingly favors IV ketamine for raw efficacy. A 2023 meta-analysis by Stevan Nikolin and colleagues, covering 49 randomized controlled trials and 3,299 participants, found that high-dose racemic ketamine produced a standardized mean difference of -0.73 on depression severity, compared to -0.48 for high-dose esketamine. Researchers at Mass General Brigham ran a naturalistic comparison of 153 patients at McLean Hospital: IV ketamine achieved a 49.22% reduction in depression scores versus 39.55% for intranasal esketamine, with IV patients improving after the first treatment rather than the second.
| Feature | IV ketamine (racemic) | Esketamine (Spravato) |
|---|---|---|
| FDA status for depression | Off-label | Approved (2019) |
| Administration | IV infusion, 40 min | Nasal spray |
| Monitoring required | During infusion + recovery | Minimum 2 hours (REMS) |
| Depression score reduction | 49.22% | 39.55% |
| Meta-analysis SMD (high dose) | -0.73 | -0.48 |
| Insurance coverage | Rarely covered | Partial coverage possible |
| Where available | Independent clinics, hospitals | REMS-certified facilities only |
Those numbers don't settle the question, though. Esketamine has longer-term data from large clinical trials. The SUSTAIN-1 trial tracked patients who had achieved remission on esketamine and found that 26.7% relapsed on continued esketamine versus 45.3% on placebo. The median time to relapse was 635 days for patients staying on esketamine compared to 88 days for those switched to placebo. That's a real maintenance benefit.
A safety study of over 800 patients on esketamine showed a 43% remission rate at 12 months. For context, patients whose depression had failed two prior antidepressants had only a 5% chance of remission at 12 months trying a third conventional medication. Esketamine also carries regulatory infrastructure — certified facilities, mandatory monitoring, adverse event reporting — that IV ketamine clinics may or may not replicate on their own.
The practical decision often comes down to insurance and access. Esketamine may qualify for partial insurance coverage because it's FDA-approved. IV ketamine is almost always out-of-pocket. Robert Meisner, medical director of McLean Hospital's Ketamine Service, put it plainly: "We always strive to seek evidence-based, data-driven, safety-first care when we consider these two treatment options."
What happens during a ketamine session
A ketamine session feels more like a supervised medical procedure than picking up a prescription. There are IV lines, vital signs checks, and some unusual perceptual effects.
For IV ketamine, you sit or recline in a treatment room. A nurse places an IV line, usually in the back of your hand. The standard dose is 0.5 mg/kg infused over 40 minutes, well below anesthetic levels (those run 1-3 mg/kg). You stay conscious the entire time. The total visit typically runs about 2.5 hours including setup and monitoring.
During the infusion, most people experience some degree of dissociation — the feeling that your mind and body are operating independently. Oxford Health NHS Foundation Trust, which runs one of the UK's largest ketamine clinics, describes the range: about 10% of patients have a "very challenging" experience, with possible anxiety, panic, or disorientation. Of the remaining 90%, roughly half find it pleasant (floating sensations, altered perception) and half feel relatively neutral. The challenging experiences almost always resolve within 15 minutes of stopping the infusion.
A typical initial treatment course involves six infusions, usually spread over two to three weeks (two or three per week). After the initial series, maintenance infusions — if the treatment works — might happen monthly or less frequently. No standardized maintenance protocol exists yet; clinicians adjust based on individual response.
| Timeline | What to expect |
|---|---|
| First 5-10 min | IV placement, vital signs check |
| 10-50 min | Infusion running; dissociative effects begin around 10-15 min |
| 50-90 min | Infusion complete; effects gradually wear off |
| 90-150 min | Recovery monitoring; most side effects resolve |
| Same day | Cannot drive; need someone to take you home |
| Next 24-72 hours | Peak antidepressant effect |
For esketamine (Spravato), the process differs. You self-administer the nasal spray under medical supervision. Dosing starts at 56 mg and may increase to 84 mg. You then stay in the clinic for at least two hours while staff monitor your blood pressure, mental state, and coordination. The FDA requires this monitoring through the REMS program — you cannot take esketamine home.
Side effects during treatment typically resolve within 1-2 hours. You shouldn't drive for 24 hours afterward. Many patients bring a book, music, or an eye mask. Some clinics offer a calming environment with dim lighting and comfortable seating; others are more clinical. The atmosphere doesn't affect the drug's efficacy, but it can influence comfort. About 50% of patients who try ketamine find enough benefit to continue with ongoing treatment.
The real cost of ketamine therapy
Ketamine therapy is expensive, and most of that cost comes out of your pocket.
A single IV ketamine infusion typically costs $400-$800. Harvard Health's Peter Grinspoon reports about $600 per infusion in the Boston area. JHU pharmacoepidemiologist Caleb Alexander notes that cash clinics charge anywhere from $500 to $1,500 per infusion, and that clinics can purchase a vial for less than $100. The markup is substantial.
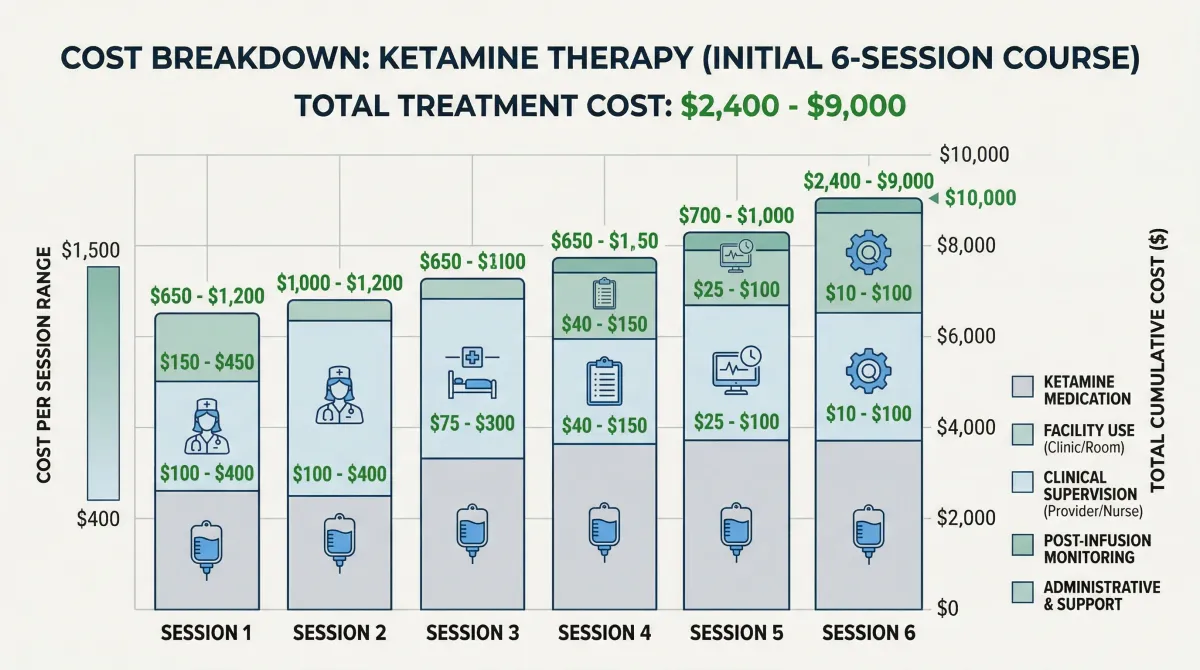
| Cost component | Typical range | Notes |
|---|---|---|
| Single IV infusion | $400-$800 | Up to $1,500 at high-end clinics |
| Initial course (6 infusions) | $2,400-$4,800 | Over 2-3 weeks |
| Monthly maintenance | $400-$800/month | Frequency varies by patient |
| Esketamine (Spravato) | Varies | May qualify for insurance; copay assistance programs exist |
| Initial consultation | $150-$350 | Separate from infusion cost at most clinics |
Insurance coverage is the dividing line. Insurance rarely covers IV ketamine because it's used off-label for depression. Esketamine, being FDA-approved, may get partial coverage, though prior authorization requirements and copays can still be steep. Some manufacturers offer copay assistance cards, and a few employer-sponsored plans have started covering esketamine. But for most patients, ketamine treatment means paying cash.
A full initial course of six infusions at typical prices runs $2,400 to $4,800. If you respond and need monthly maintenance, add $4,800 to $9,600 per year. That's real money, particularly for patients who have already spent thousands on medications that didn't work. When evaluating cost, factor in consultations (often $150-$350 for the initial evaluation), transportation (you can't drive yourself), and time off work for the 2-3 hour appointments.
Finding a reputable ketamine provider
Hundreds to thousands of ketamine clinics now operate across the United States, and quality varies enormously. Some are university-affiliated programs with rigorous protocols. Others are cash-only storefronts with minimal oversight.
For esketamine (Spravato), finding a provider is more straightforward: treatment can only happen at REMS-certified healthcare facilities. The manufacturer (Janssen) maintains a provider locator. These sites must have trained staff, monitoring protocols, and adverse event reporting systems.
For IV ketamine, the search requires more work. When Harvard Health's Peter Grinspoon called several clinics posing as a patient, he found that most "seemed as if they would provide ketamine for me without any major hurdles, after an introductory medical interview by a nurse or a social worker." Only a few required communication with his existing psychiatrist.
What to look for in a ketamine provider: A psychiatrist or anesthesiologist on staff who manages treatment. A thorough intake evaluation including psychiatric history, medication review, and screening for contraindications. Communication with your existing mental health providers. Vital sign monitoring during and after treatment. Clear protocols for managing adverse reactions. Willingness to discuss the limits of current evidence.
Be cautious of clinics that guarantee results, minimize risks, advertise ketamine for conditions with weak evidence (Lyme disease, autoimmune disorders), or offer at-home compounded ketamine without adequate supervision. The FDA issued a specific warning in October 2023 about compounded ketamine products from telemedicine platforms, noting that these products "are not FDA approved, which means FDA has not evaluated their safety, effectiveness, or quality." JHU's Caleb Alexander was blunter: offering compounded ketamine as a nasal spray for at-home use is "just bonkers" because dose standardization is nearly impossible.
Academic medical centers and hospital-affiliated programs tend to have more safeguards. Grinspoon noted that "the ketamine clinics affiliated with medical academic institutions seem to have more safeguards in place" and may also enroll patients in clinical trials, giving access to newer protocols. That's not a requirement, but it's a useful signal.
One safety data point: a prospective study tracking 1,148 patients receiving esketamine under REMS found zero reports of patients seeking, misusing, or overdosing on the drug. The REMS framework — supervised administration, mandatory monitoring, structured reporting — works. When choosing an IV ketamine provider, look for clinics that voluntarily adopt similar standards.
Risks, side effects, and who should skip it
Ketamine's side effect profile at antidepressant doses is manageable for most people, but it's not trivial. The most common effects during and shortly after treatment include dissociation, elevated blood pressure, dizziness, nausea or vomiting, headache, blurred vision, anxiety, and sedation. These are reported consistently across sources — Harvard Health, the Oxford NHS ketamine clinic, the PMC review by Zarate and colleagues, and the UK government's Advisory Council on the Misuse of Drugs all document the same pattern.
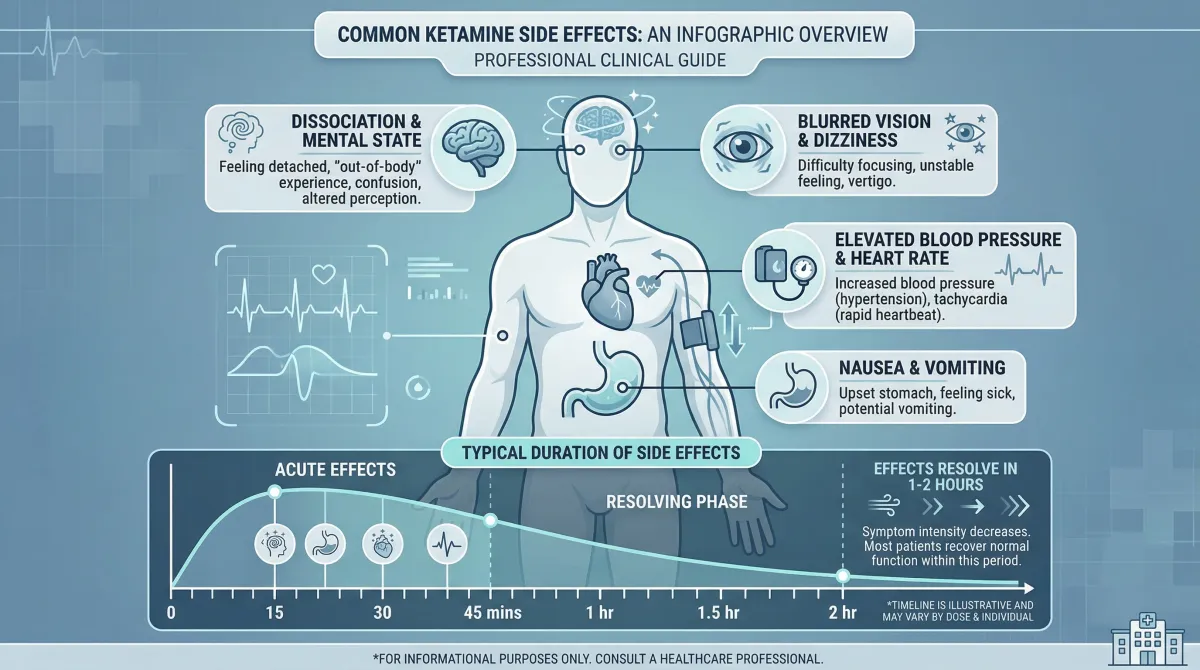
Side effects typically resolve within 1-2 hours of treatment. The more serious concern is what we don't know about long-term use.
Multiple authoritative sources — Harvard Health, Yale Medicine's Gerard Sanacora, the PMC clinical review, and the BJPsych Open guidelines — flag that long-term effects of repeated ketamine treatment are not well studied. No large-scale, long-term studies exist for racemic IV ketamine in psychiatric use. This is the biggest gap in the evidence.
From recreational ketamine users (who take dramatically higher doses), we know that bladder damage is common at doses above 1 gram daily — far exceeding the roughly 35-50 mg used in a typical antidepressant infusion for a 70 kg person. The UK government's 2024-2025 data shows 264,000 estimated recreational users and a 12-fold increase in treatment referrals for ketamine use disorders since 2015. Clinical doses and recreational doses are different animals, but the recreational misuse data explains why regulators are cautious.
Tolerance is another concern. Oxford NHS reports that some patients find their depression returns despite continuing treatment, which may indicate tolerance. In those cases, the clinic may extend intervals between doses, raise the dose cautiously, or add a low oral dose between infusions. Sometimes ketamine simply stops working for a given patient.
Some groups should avoid ketamine therapy entirely. Harvard Health identifies the following contraindications:
- History of psychosis or schizophrenia — dissociation can worsen psychotic disorders
- Active substance use disorder — ketamine triggers opioid receptors and can cause euphoria; addiction risk is real
- Pregnancy or breastfeeding — insufficient safety data
- Adolescents — concerns about effects on the developing brain; only one small study of 17 adolescents exists
- Older adults with dementia symptoms — cognitive effects may compound existing impairment
Cleveland Clinic psychiatrist Brian Barnett highlights a particular challenge for patients with co-occurring depression and substance use disorders: "Many ketamine clinical trials have either required extended abstinence or excluded patients with SUDs altogether. This leaves us with a limited understanding of which SUDs pose the greatest risk of ketamine misuse." The death of actor Matthew Perry — who had a history of substance use disorder and became addicted to ketamine prescribed for depression — underlines this risk.
Ketamine therapy isn't reckless when done right, but "done right" means medical supervision, honest conversations about what isn't yet known, and careful patient selection. The BJPsych Open clinical guidelines recommend national registries to track long-term outcomes and adverse events systematically.
Frequently asked questions
How quickly does ketamine work for depression?
Antidepressant effects can begin within 40 minutes of an IV infusion, with peak improvement around 24 hours. Traditional antidepressants typically take 4-6 weeks. A single dose's effects last 3-7 days, which is why repeated treatments are needed.
Is ketamine FDA-approved for depression?
Ketamine itself is not FDA-approved for any psychiatric disorder. It's approved only as an anesthetic. Esketamine (the S-enantiomer, brand name Spravato) received FDA approval in 2019 for treatment-resistant depression and in 2020 for major depression with suicidal ideation. IV ketamine is used off-label for depression, which is legal but means it hasn't gone through the FDA's formal review process for this use.
Can I get ketamine therapy through my insurance?
Insurance rarely covers IV ketamine since it's off-label. Esketamine (Spravato) has a better chance of partial insurance coverage because it's FDA-approved, though prior authorization is typically required. Most IV ketamine clinics operate on a cash-pay basis. A full initial treatment course of six infusions can cost between $2,400 and $9,000 depending on your location and clinic.
Is at-home ketamine safe?
The FDA issued a specific warning in October 2023 about compounded ketamine products marketed by telemedicine platforms for at-home use. Without on-site medical monitoring, patients face increased risks from sedation, dissociation, and blood pressure changes. The FDA reported a case where a patient taking compounded oral ketamine at home had blood levels twice the anesthetic threshold. Clinical experts consistently recommend in-person administration with medical supervision.
What's the difference between ketamine and esketamine?
Ketamine (racemic) contains two mirror-image molecules (R and S enantiomers). Esketamine is just the S-enantiomer and is more potent at the NMDA receptor. IV racemic ketamine shows numerically greater efficacy in meta-analyses and faster onset, but esketamine has FDA approval, more regulatory oversight, and better chances of insurance coverage. The right choice depends on your clinical situation, insurance, and access.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.