
The Word "Bioidentical" Means Less Than You Think
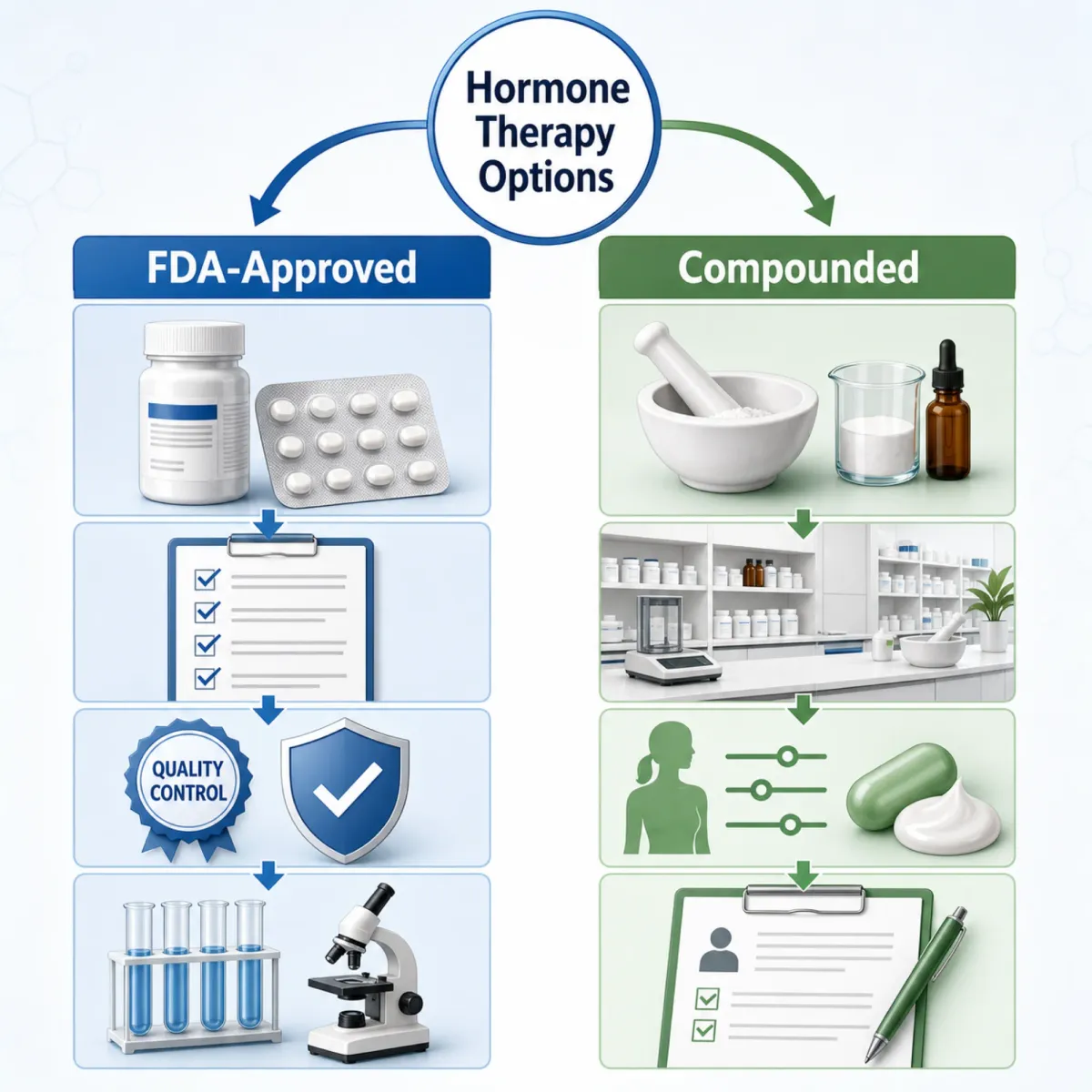
Walk into any anti-aging clinic and you will hear "bioidentical" used as though it automatically means safer. The actual definition is narrower: a bioidentical hormone has a chemical structure matching what your ovaries once produced. The term says nothing about where it was made, how it gets delivered, or whether anyone tested it for safety.
This distinction matters because two very different products get called bioidentical. On one side are FDA-approved bioidentical hormones like estradiol patches (Vivelle-Dot, Climara), oral estradiol (Estrace), and micronized progesterone (Prometrium). These went through clinical trials, batch consistency testing, and carry labeled warnings about known risks. On the other side are compounded bioidentical hormones (cBHT) mixed by compounding pharmacies into custom creams, troches, and pellets. These skip the FDA approval process entirely.
A National Academies report found that between 1.0 and 2.5 million American women over 40 use compounded bioidentical hormones, generating roughly 26 to 33 million prescriptions and $1 to $2 billion in annual spending. About one-third of all hormone therapy users chose compounded products over FDA-approved versions.
Marketing plays a substantial role in their popularity. That same National Academies analysis found 65% of cBHT clinic websites claimed reduced breast cancer risk or protective effects. Among users surveyed, 77% believed compounded hormones were safer than conventional therapy, and 86% did not know whether their compounded product was FDA-approved.
Every major medical organization in the field disagrees with those marketing claims. The Menopause Society states that custom-compounded hormones are "not safer or more effective than approved bioidentical hormones." The American College of Obstetricians and Gynecologists, the Endocrine Society, and the American Medical Association have all issued similar positions. The National Academies committee "could not identify any specific life-threatening medical conditions requiring the patient's use of cBHT preparations."
Compounded products do serve a narrow legitimate role: for women with documented allergies to inactive ingredients in FDA-approved formulations, or when a specific dose has no commercially available equivalent. Outside those cases, the evidence does not support choosing compounded over regulated products. If your provider recommends a compounded formulation, ask whether an FDA-approved bioidentical option exists first.
Decades of Data: What Hormone Therapy Actually Does
The Women's Health Initiative is the largest randomized controlled trial ever conducted on hormone therapy. Launched in 1993, it enrolled more than 68,000 postmenopausal women with follow-up lasting up to 20 years. When the combined estrogen-plus-progestin arm was stopped early in 2002 because breast cancer cases exceeded safety limits, US prescriptions fell an estimated 80% within seven years.
The original WHI headlines were alarming but incomplete. The combined therapy arm (conjugated equine estrogens plus medroxyprogesterone acetate) showed increased risks for breast cancer (hazard ratio 1.26), coronary heart disease (1.29), stroke (1.41), and venous thromboembolism (2.13). What received far less attention: the estrogen-only arm told a different story. Twenty-year follow-up data showed that estrogen-only therapy actually decreased both the incidence and mortality of breast cancer compared to placebo.
Two decades of reanalysis have produced a more nuanced picture. The timing hypothesis, now widely accepted, shows that benefits outweigh risks when hormone therapy starts within 10 years of menopause onset or before age 60. The WHI participants averaged 63 years old at enrollment, well past the window where most women actually begin HRT. A 2024 review in JAMA led by JoAnn Manson concluded that women under 60 with low-to-average cardiovascular and breast cancer risk who want symptom relief may experience net benefits.
The proven benefits are substantial. The Menopause Society calls hormone therapy "the most effective treatment" for vasomotor symptoms like hot flashes and night sweats. A meta-analysis found that both oral and transdermal estrogens reduce the risk of hip, vertebral, and total fractures by 20 to 37%. Cardiovascular data from longer follow-up shows estrogen monotherapy in women past 65 associated with a 19% reduction in overall mortality (adjusted hazard ratio 0.81), along with reductions in heart attack and heart failure incidence.
Not all delivery methods carry equal risks. Oral estrogen undergoes first-pass liver metabolism, which increases clotting factors, triglycerides, and inflammatory markers. Transdermal estrogen (patches, gels) bypasses the liver and avoids those effects. For women over 60 or those with clotting risk factors, transdermal delivery paired with micronized progesterone is considered the safer configuration.
The type of progestogen matters too. Data from a French cohort study showed micronized progesterone carried a breast cancer relative risk of 1.0 compared to 1.69 for synthetic progestins. This is why the shift toward bioidentical estradiol and micronized progesterone is not just marketing. For this particular combination, the evidence genuinely favors it over the older conjugated estrogen plus synthetic progestin protocols the WHI studied.
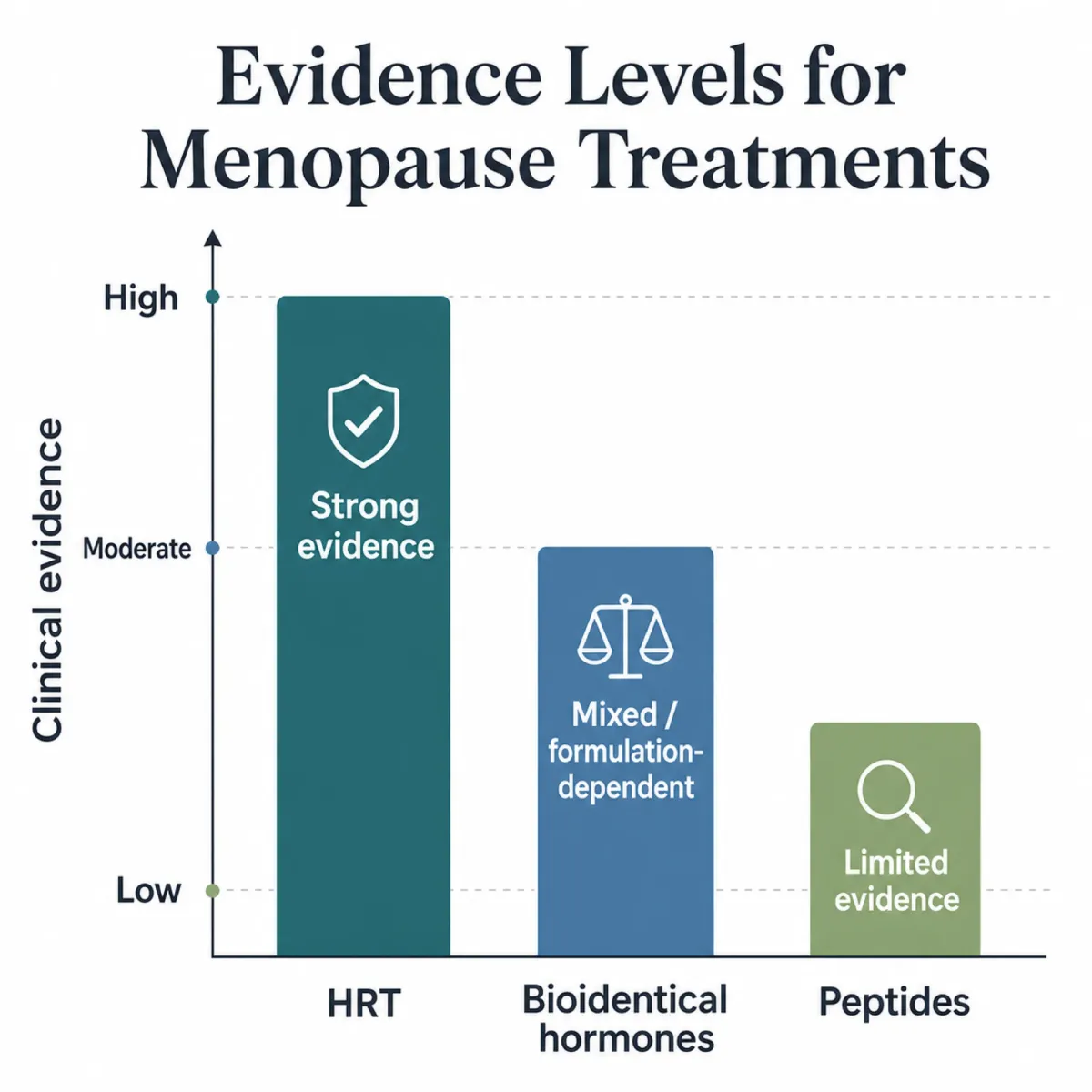
Peptides for Menopause: Promising Biology, Thin Evidence
Peptide clinics market a growing list of compounds for menopausal women: growth hormone secretagogues for body composition, BPC-157 for joint pain, kisspeptin for hormonal regulation, PT-141 for libido. The biological rationale for each ranges from plausible to genuinely interesting. The clinical evidence, with one exception, does not match the marketing.
Consider BPC-157, the most heavily promoted peptide for tissue repair. A systematic review screened 544 papers and found only 1 of 36 included studies involved humans in a musculoskeletal context. The human data that exists is a retrospective study of 16 knee-pain patients, a pilot study of 12 women with interstitial cystitis, and an intravenous safety study of 2 healthy adults. These numbers are "too small and poorly controlled to establish whether the peptide outperforms natural recovery, the placebo effect, or conventional rehabilitation." The FDA classified BPC-157 as not eligible for 503A compounding as of April 2026, citing adverse immune system reactions and insufficient safety data.
Growth hormone secretagogues like CJC-1295 and ipamorelin have stronger mechanistic data but similar regulatory problems. A 2006 study published in the Journal of Clinical Endocrinology and Metabolism showed CJC-1295 produces sustained, dose-dependent GH increases of 2 to 10 fold lasting 6 or more days after a single injection. Ipamorelin offers a cleaner pharmacological profile, selectively stimulating growth hormone release without triggering cortisol or prolactin at 200 times its effective dose. But the CJC-1295 Phase 2 trial was discontinued after a participant death (deemed unrelated), and neither compound has Phase 3 data in any population. The FDA's Pharmacy Compounding Advisory Committee voted against Category 1 inclusion for both, and their compounding eligibility remains contested.
The lone exception in the peptide lineup is PT-141 (bremelanotide), marketed as Vyleesi. It went through proper Phase 3 trials, with the RECONNECT studies enrolling roughly 1,247 women and demonstrating statistically significant improvements in sexual desire. It earned FDA approval in 2019. The catch: approval is only for hypoactive sexual desire disorder in premenopausal women. Postmenopausal use remains off-label.
The safety concerns extend beyond individual compounds. Dr. Sarah Bonza, a board-certified family physician and Menopause Society Certified Practitioner, flags that multiple peptides activate pathways tumors exploit. IGF-1 elevation from growth hormone secretagogues is consistently linked to increased cancer risk in epidemiological studies. BPC-157 activates VEGF/VEGFR2 pathways that are active in roughly half of human cancers. A 2026 review in Frontiers in Aging confirmed that "long-term safety data in elderly populations are virtually absent for non-approved peptides" and that "optimal dosing regimens remain poorly defined for most peptides."
There is a useful concept from drug development called the translational squeeze. Only about 1 in 20 compounds that show promise in rodent studies successfully reach human trials and regulatory approval. Peptide marketing tends to present animal data as though it directly predicts human outcomes. It does not.
Head-to-Head: Putting the Numbers Side by Side
| Factor | FDA-Approved Bioidentical HRT | Peptide Therapy |
|---|---|---|
| Evidence base | 68,000+ women in WHI; decades of RCTs, meta-analyses, long-term follow-up | Mostly preclinical; largest human peptide studies: 12-58 patients in pilots |
| FDA approval for menopause | Yes (estradiol, micronized progesterone, multiple formulations) | No peptide approved for menopause symptoms (PT-141 approved for premenopausal HSDD only) |
| Vasomotor symptom relief | Proven. "Most effective treatment" per Menopause Society | Not established in human trials |
| Bone protection | 20-37% fracture risk reduction (meta-analysis) | Theoretical (GH secretagogues); no human fracture data |
| Insurance coverage | Most plans cover FDA-approved HRT | Not covered; 100% out-of-pocket |
| Monthly cost (with insurance) | $10-$40/month for generic pills or patches | $200-$500+/month (no insurance option) |
| Monthly cost (without insurance) | $50-$319/month depending on delivery method | $200-$500+/month plus labs |
| Regulatory oversight | FDA-regulated manufacturing, labeled warnings, adverse event reporting | Most compounds not eligible for legal compounding as of 2026 |
| Long-term safety data | 20+ years of follow-up data from WHI and other trials | "Virtually absent" per 2026 Frontiers in Aging review |
The cost gap deserves specific attention. Generic estradiol pills run less than $10 for a 90-day supply. Patches with insurance coverage stay under $40 per month. Micronized progesterone (generic Prometrium) costs less than $20 for a 90-day supply. A woman paying out of pocket for generic oral HRT might spend $15 to $30 per month total.
Peptide therapy operates entirely outside insurance. Growth hormone secretagogues, BPC-157 vials, and associated prescriber visits and lab monitoring typically run $200 to $500 or more per month. Annual costs for peptide therapy with proper medical oversight easily reach $3,000 to $6,000, none of it reimbursable. The National Academies noted that average out-of-pocket cost for compounded hormones was $88 per prescription versus $49 for FDA-approved versions, and total annual compounded costs including testing and visits ranged from $1,400 to $3,500.
That is a meaningful financial commitment for compounds where, as one researcher framed it, "plausible biology can generate excitement long before it generates reliable clinical evidence."
The Combination Question: Why Clinics Offer Both
A growing number of longevity and functional medicine clinics offer HRT and peptides as a combined protocol. The rationale is that menopause involves two overlapping hormonal declines. Estrogen and progesterone drop during menopause itself, while growth hormone and IGF-1 decline gradually with age in a process called somatopause. Mandelli and colleagues documented in a 2022 Climacteric paper that concurrent estrogen loss and somatopause compound bone and muscle decline into a condition called osteosarcopenia. HRT addresses the first decline; growth hormone secretagogues theoretically address the second.
The logic extends beyond body composition. Some women on otherwise well-managed HRT still experience persistent joint pain, residual sleep disruption, or skin changes that estrogen replacement does not fully resolve. Clinics position peptides like BPC-157 for musculoskeletal complaints, collagen peptides for skin thickness, and kisspeptin as a research-stage compound targeting HPG axis dimensions that estrogen alone may not normalize.
The evidence gap here is significant. No completed human randomized controlled trial has studied any peptide compound specifically as an adjunct to HRT in menopausal women as of April 2026. The combination approach rests on biological plausibility and clinical observation from individual practices. The 2026 Frontiers in Aging review was explicit: "effects of combination therapy are unexplored" in the published literature.
Medicine often operates at the edge of evidence, particularly for conditions where standard treatments leave residual symptoms. But you should understand what you are paying for: a biologically reasonable hypothesis, not a clinically validated protocol. Any provider presenting peptide-HRT combinations as established medicine is overstating what the research supports.
Making the Decision: Who Benefits from What
For most symptomatic women within 10 years of menopause, FDA-approved hormone therapy should be the starting point. The symptom relief is proven, the costs are manageable, and the risk profile is well-characterized after decades of study. The Menopause Society, ACOG, and the Endocrine Society all support this position for appropriate candidates.
Several groups face legitimate barriers to standard HRT. Women with a history of breast cancer, uterine cancer, unexplained uterine bleeding, liver disease, prior blood clots, or active cardiovascular disease have relative or absolute contraindications. For these women, the conversation about alternatives is real and necessary. Non-hormonal options like fezolinetant (a neurokinin-3 receptor antagonist) have emerged with proper clinical trials behind them. Peptides occupy a different category: possibly helpful for specific complaints, but without the controlled data to recommend them as HRT replacements.
Women considering peptides should also understand the contraindications specific to those compounds. Dr. Bonza lists current or recent cancer diagnosis, strong family history of hormone-sensitive cancers, BRCA1/2 mutations, active autoimmune disease, and pregnancy as contraindications for most injectable peptides. Growth hormone secretagogues are contraindicated in active insulin resistance or type 2 diabetes because they affect glucose metabolism.
A practical framework for the decision: Start with established hormone therapy if you are a candidate. If HRT resolves your symptoms, you likely do not need peptides. If specific complaints persist despite optimized HRT, discuss targeted peptide options with a provider who is transparent about the evidence gaps. If you cannot take HRT, explore FDA-approved non-hormonal alternatives before turning to unregulated peptides.
Dr. Bonza requires a prerequisite checklist before she will even discuss peptides with patients: hormonal optimization first, nutritional deficiency correction, nervous system regulation, and lifestyle foundations including strength training, adequate protein, and 7 to 8 hours of sleep. As she puts it: "Peptides are not a replacement for foundational health. They are not a shortcut, not a magic solution, and certainly not appropriate for everyone."
Half of all women experience symptom recurrence after stopping hormone therapy. Whatever path you choose, plan for ongoing evaluation rather than a one-time decision.
Frequently Asked Questions
Are bioidentical hormones the same as compounded hormones?
No. "Bioidentical" describes a hormone's chemical structure matching what your body produces. Both FDA-approved products (like Estrace and Prometrium) and compounded pharmacy preparations can be bioidentical. The difference is regulatory oversight: FDA-approved versions undergo clinical trials and batch testing, while compounded versions do not. The Menopause Society and National Academies recommend FDA-approved bioidentical options over compounded ones when available.
Can peptides replace hormone therapy for menopause symptoms?
The evidence does not support this. As of 2026, no peptide is FDA-approved for menopause symptom management. HRT has decades of randomized controlled trial data proving it relieves hot flashes, prevents bone fractures, and addresses vaginal atrophy. Peptides have mostly preclinical or small pilot study data. Women who cannot take HRT should discuss FDA-approved non-hormonal alternatives like fezolinetant with their providers before considering unregulated peptides.
How much does peptide therapy cost compared to HRT?
Generic FDA-approved HRT can cost as little as $10 to $40 per month with insurance. Peptide therapy typically runs $200 to $500 or more per month entirely out-of-pocket since insurance does not cover it. Annual peptide therapy costs with proper medical oversight and lab monitoring can reach $3,000 to $6,000.
Is it safe to use peptides alongside hormone therapy?
No randomized controlled trial has studied the safety of any peptide-HRT combination in menopausal women. Some clinics offer combined protocols based on biological plausibility and clinical observation, but this approach lacks controlled evidence. Women with cancer risk factors, insulin resistance, or autoimmune conditions should be particularly cautious about adding growth hormone secretagogues to their HRT regimen.
What should I try first for menopause symptoms?
Medical guidelines consistently recommend FDA-approved hormone therapy as the first-line treatment for moderate-to-severe vasomotor symptoms in eligible women within 10 years of menopause. Transdermal estradiol with micronized progesterone carries the most favorable risk profile based on current evidence. Peptides should be considered only after HRT has been optimized and specific residual symptoms persist.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











