
What Hormone-Friendly Means After 50
For women past midlife, the first question is not """which peptide is strongest?""" It is """which one is least likely to fight my hormones, my cancer history, my glucose, or my sleep?""" That filter changes the list fast.
Menopause is a normal aging stage, not a disease, and it means menstrual periods have stopped permanently according to the National Institute on Aging. Most women begin the menopausal transition between ages 45 and 55, and the average age of menopause in the United States is 52 according to the same NIA guide. During that transition, estrogen and progesterone decline greatly as the NIA explains.
That hormone shift can show up as hot flashes, night sweats, trouble sleeping, joint and muscle discomfort, pain during sex, moodiness, forgetfulness, and difficulty concentrating the NIA notes. It can also change energy use, fat distribution, bone density, heart health, body shape, body composition, and physical function during the menopausal transition.
Think of hormones like the main electrical panel in a house. A peptide is more like a doorbell wire or thermostat signal: smaller, targeted, and still capable of causing trouble if wired into the wrong system. """Hormone-friendly""" should mean low systemic disruption, clear evidence for the goal, realistic monitoring, and no promise that a peptide replaces individualized menopause care.
A hormone-friendly peptide is not automatically """natural""" or safe. It earns that label only when the benefit is specific, the systemic hormone impact is limited, and the monitoring plan is boringly clear.

The Best-Supported Options Are Not the Flashiest
The least dramatic candidate is also the easiest to discuss conservatively: oral collagen peptides. Collagen peptides are not HRT. They do not fix hot flashes. They do not """balance hormones.""" They sit in a narrower lane: skin structure support.
In a randomized, double-blind, placebo-controlled trial, E. Proksch and colleagues assigned 69 women aged 35 to 55 to 2.5 g collagen hydrolysate, 5.0 g collagen hydrolysate, or placebo once daily for 8 weeks in Skin Pharmacology and Physiology. Skin elasticity improved significantly versus placebo in both collagen dosage groups, while moisture and evaporation findings in subgroup analysis did not reach statistical significance in the PubMed abstract. No side effects were noted throughout the study according to the trial abstract.
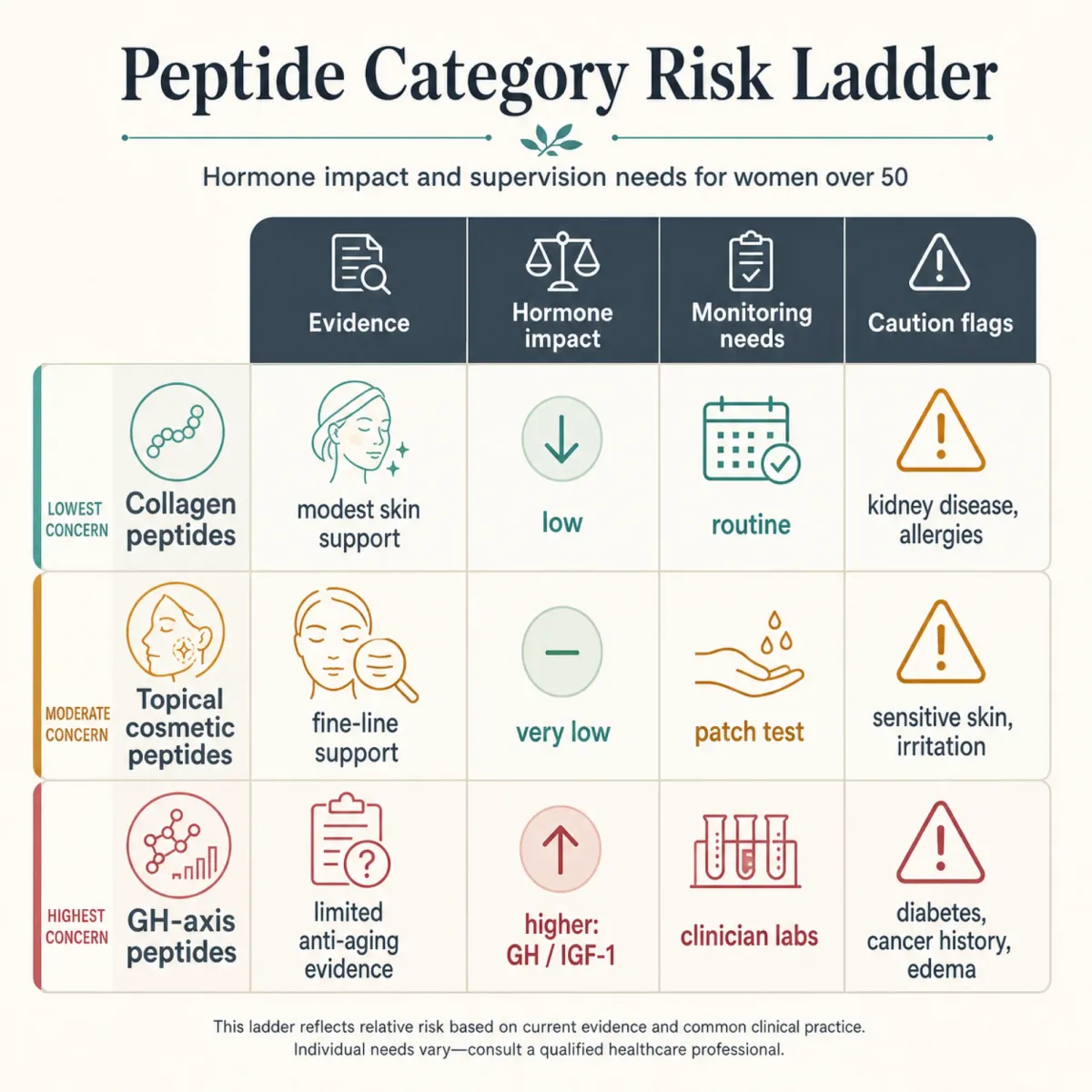
| Peptide category | Hormone impact | Best-fit goal | Conservative take |
|---|---|---|---|
| Oral collagen peptides | Low systemic hormone impact | Skin elasticity | Reasonable first discussion if supplement quality is solid |
| Topical cosmetic peptides | Usually lower than injectables | Skin barrier and appearance | Judge product claims carefully |
| GH-axis peptides | Higher endocrine involvement | Body composition or visceral-fat claims | Needs clinician oversight and labs |
| Experimental longevity peptides | Unclear | Telomere, sleep, brain-aging claims | Not a routine menopause protocol |
The practical point is simple: a peptide that helps one skin metric in one controlled study is not a blank check. It is more like a small repair crew replacing weather stripping. Useful, maybe. But it is not rebuilding the whole house.
This is also why """hormone-friendly""" should not be a vibe word. It should answer three plain questions: does the peptide directly push a hormone pathway, does the evidence match the goal, and would stopping it be easy if symptoms or labs move the wrong way? Collagen peptides pass more of that test than most injectable anti-aging stacks because the claim is narrower and the endocrine footprint is smaller.
Skin, Hair, and Barrier Peptides: Where the Evidence Is Cleanest
Skin is where many women first notice aging, and it is also where peptide claims are easiest to overstate. The collagen trial gives a credible, modest anchor: elasticity improved, but not every skin endpoint became statistically significant in Proksch and colleagues' trial. That is a useful distinction because """better elasticity""" is not the same as """reversed menopause skin aging."""
Copper peptides such as GHK-Cu and AHK-Cu are often marketed for skin and hair. In this research run, however, the strongest primary GHK-Cu sources were blocked by anti-bot pages, and the accessible support was mainly lower-authority clinic material. That does not prove the peptides do not work. It means they should be discussed as cosmetic-interest peptides, not as proven postmenopausal anti-aging therapy.
The FDA's menopause page offers the right attitude for this category: check online information, ask a health care provider about risks and benefits, and remember that natural does not always mean safe as the FDA advises. That applies to serums, powders, compounded injectables, and """bioidentical""" claims alike.

For a woman over 50, the safer skin-peptide question is not """what gives the fastest lift?""" It is """what has human evidence, what touches systemic hormones, and what would I stop if my skin, sleep, glucose, or breast-health plan changed?"""
Muscle, Recovery, and Metabolic Peptides Need a Different Standard
Muscle and metabolic aging are where peptide conversations become more medically serious. The reason is the growth hormone axis. Once a peptide is trying to raise GH or IGF-1, it is no longer just a beauty product. It is pressing on a system tied to glucose, fluid retention, tissue growth, and sometimes cancer caution.
Hau Liu and colleagues reviewed 31 articles representing 18 unique study populations of GH therapy in healthy elderly adults in Annals of Internal Medicine. The review included 220 GH-treated participants, with mean age 69 and mean BMI 28 kg/m2 in the same review. GH therapy decreased fat mass by 2.1 kg and increased lean body mass by 2.1 kg, while weight did not change significantly Liu and colleagues reported.
That chart looks tempting until you read the safety line. GH-treated participants were more likely to experience soft tissue edema, arthralgias, carpal tunnel syndrome, and gynecomastia, and were somewhat more likely to experience diabetes mellitus onset and impaired fasting glucose in the Liu review. The authors concluded that GH cannot be recommended as anti-aging therapy based on that evidence.
Tesamorelin sits in this same caution zone. It is described as a synthetic 44-amino-acid GHRH analogue that increases GH and IGF-1 through pituitary signaling in the fetched clinical explainer. WADA's prohibited list includes growth hormone analogues and fragments, GHRH analogues such as CJC-1295, sermorelin, and tesamorelin, plus growth hormone secretagogues such as ibutamoren and ipamorelin in its peptide hormones section.
The practical implication: if the peptide is meant to change muscle, recovery, visceral fat, or IGF-1, treat it like endocrine medicine. Ask what diagnosis it is treating, what lab will prove it is appropriate, what lab will trigger stopping, and why the goal cannot be addressed first with resistance training, protein, sleep, approved menopause care, or cardiometabolic treatment.
That does not mean every GH-axis discussion is reckless. It means the standard should be higher than """I feel older.""" In a woman with menopause-related sleep disruption, joint pain, changing body composition, and a family history of breast cancer, the same peptide can look very different than it does in a generic longevity brochure. Context is the medicine.
Sleep, Libido, and Brain-Aging Peptides: Promising Is Not the Same as Ready
Sleep, libido, and cognition matter enormously after menopause. The NIA lists trouble sleeping, pain during sex, mood changes, forgetfulness, and difficulty concentrating among symptoms some women experience during the menopausal transition in its menopause guide. That is exactly why this category attracts bold peptide marketing.
But bold marketing is not the same as clinical readiness. DSIP, PT-141, kisspeptin, and epitalon came up in the research corpus, yet the accessible fetched evidence did not support presenting them as established anti-aging protocols for postmenopausal women. In practical terms, this is the yellow-light shelf: interesting mechanisms, narrow indications or weak evidence, and too much room for clinics to sell certainty the literature has not earned.
| Goal | What to ask first | Why it matters after 50 |
|---|---|---|
| Sleep | Have hot flashes, apnea, pain, medications, alcohol, and thyroid issues been reviewed? | A peptide cannot fix a missed sleep diagnosis. |
| Libido | Is this desire, pain, dryness, relationship stress, medication effect, or mood? | Postmenopausal sexual symptoms often have more than one driver. |
| Brain aging | Is there evidence in women like me, or just animal and longevity-clinic claims? | Mechanism is not the same as outcome. |
Think of this category like a promising recipe scribbled on a napkin. It may become a real dinner someday, but you would not serve it to guests without testing it. If a clinic presents a sleep, libido, or telomere peptide as a shortcut around menopause evaluation, that is a reason to slow down.
Peptides, HRT, Cancer, and Cardiometabolic Risk
Peptides and HRT are often framed as competitors. That framing is too simplistic. HRT has a defined menopause role for selected women; peptides usually do not. Peptides may be adjuncts, cosmetic products, or off-label endocrine interventions, depending on the compound.
MedlinePlus says HRT should not be used by women who think they are pregnant, have unexplained vaginal bleeding, have had certain cancers, have had a stroke or heart attack, have had blood clots, or have liver disease in its HRT summary. It also states that some hormone therapy may increase chances of blood clots, heart attacks, strokes, breast cancer, and gallbladder disease, with risk varying by medical history and lifestyle according to MedlinePlus.
That risk list does not automatically transfer to every peptide. But it explains why women over 50 should not accept vague """hormone-friendly""" language. If a peptide raises GH, IGF-1, glucose, water retention, or tissue-growth signaling, the conversation belongs in the same careful medical file as mammography history, cancer history, clotting history, diabetes risk, blood pressure, lipids, and HRT decisions.
MedlinePlus advises using the lowest helpful HRT dose for the shortest needed time and checking every 3 to 6 months whether HRT is still needed in its hormone therapy guidance. Peptide therapy deserves a similar stop-rule mindset: define the goal, define the risk, measure both, and do not keep escalating because """anti-aging""" has no obvious finish line.
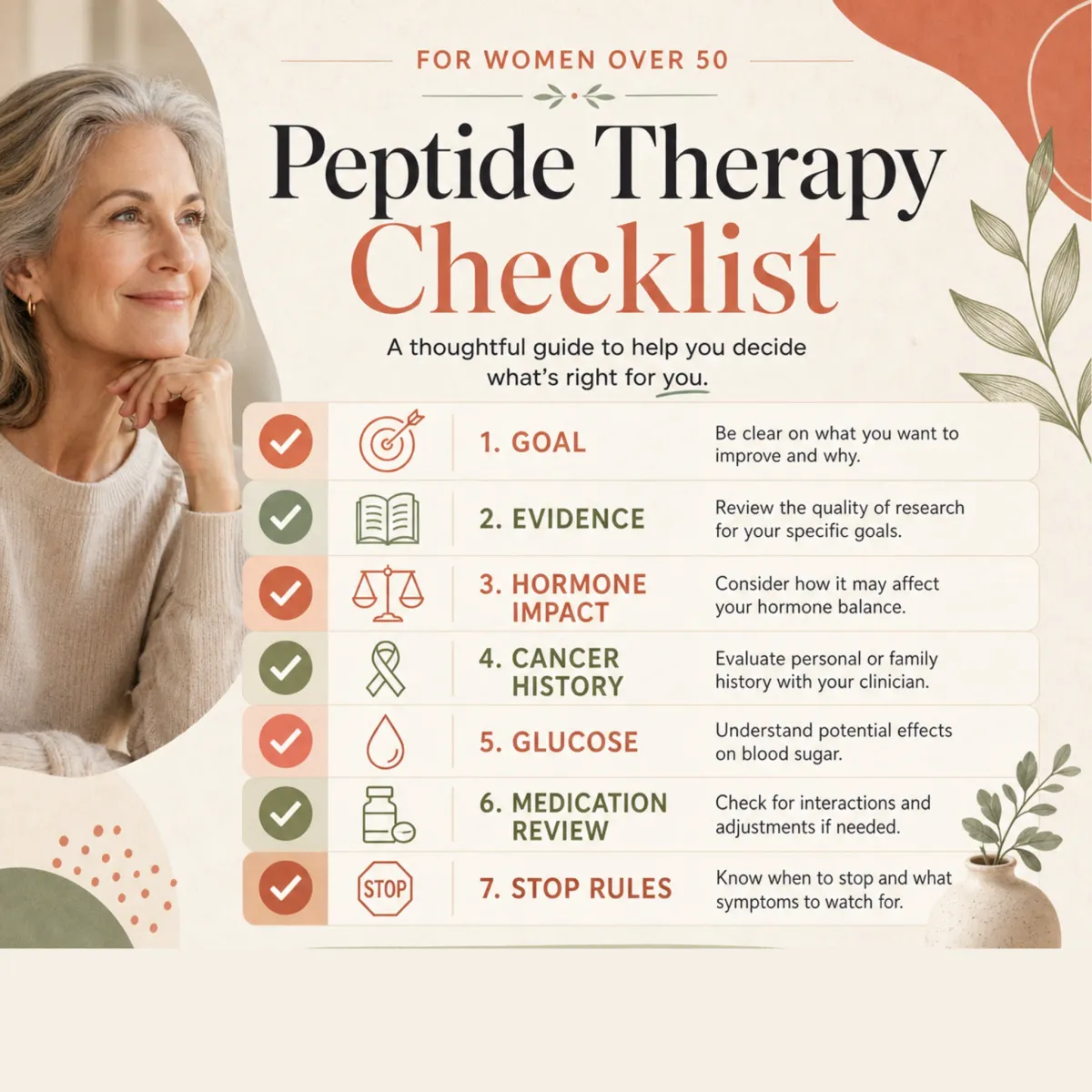
A clean clinician conversation might sound almost disappointingly practical: What symptom are we treating? What diagnosis supports this? What medication or supplement could conflict? What breast, clotting, cardiovascular, liver, glucose, and cancer-history issues change the plan? If the answer is """we do not need to check any of that,""" the protocol is not hormone-friendly. It is just under-specified.
A Conservative Shortlist to Discuss With Your Clinician
If you want the hormone-friendly version of this list, rank peptides by how little they ask of your endocrine system.
| Discussion tier | Examples | Why it belongs there | Monitoring question |
|---|---|---|---|
| Green-yellow | Oral collagen peptides | Human skin elasticity data with low hormone impact | Any allergy, supplement quality, kidney/protein restrictions, or medication concerns? |
| Yellow | Topical cosmetic peptides | Lower systemic exposure, but variable product claims | Is the product irritant-free, sunscreen-compatible, and realistic in claims? |
| Orange | Sermorelin, ipamorelin, CJC-1295, tesamorelin | GH/IGF-1 pathway involvement | What are baseline IGF-1, fasting glucose/A1c, cancer history, edema, and stop rules? |
| Red until proven otherwise | Epitalon, DSIP, BPC-157, TB-500, grey-market stacks | Insufficient direct evidence for routine postmenopausal anti-aging use | Why this compound, why now, and what evidence is in women like me? |
One fetched clinical explainer suggested reviewing peptide protocols every 8 to 12 weeks with symptom scores, labs, side effects, and dose logs in its monitoring discussion. That is lower-authority than a guideline, but the idea is sensible: if you cannot write down what you are measuring, you are not optimizing. You are experimenting.
The FDA gives the cleanest final rule: ask a health care provider what treatment is right for you, ask about risks and benefits, and avoid claims that sound too good to be true in its menopause advice. For women over 50, the hormone-friendly peptide list is short because it should be short. Skin support can be reasonable. GH-axis manipulation requires real medical supervision. Longevity stacks should earn skepticism first.
Frequently Asked Questions
Are peptides safer than HRT for women over 50?
Not automatically. HRT has known menopause indications and known risk discussions, while many peptides are cosmetic, supplemental, or off-label. A peptide may have lower hormone impact, but that does not make it safer for your cancer history, glucose, medications, or goals.
Which anti-aging peptide is most hormone-friendly?
Based on this evidence review, oral collagen peptides are the most conservative place to start because their best evidence is skin elasticity support, not systemic hormone manipulation. Even then, they are a supplement discussion, not a menopause treatment plan.
Should women over 50 avoid sermorelin, ipamorelin, CJC-1295, or tesamorelin?
They should avoid casual use. These peptides involve the GH/IGF-1 axis, so they call for clinician oversight, baseline labs, glucose monitoring, cancer-history review, and clear stop rules.
Can peptides replace menopause care?
No. Peptides should not replace individualized care for hot flashes, sleep disruption, vaginal symptoms, bone health, cardiovascular risk, or HRT decisions. Use them, if at all, as a narrow add-on with a defined goal.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











