
What Actually Changes in Perimenopause — and Why Weight Goes Up
"Your metabolism slows after 50" is technically true and clinically useless. The actual question is which biological levers move, in what order, and why the same caloric deficit that worked at 38 stops doing much at 48.
Perimenopause, per the federal Office on Women's Health, "typically begins in a woman's mid- to late 40s" and lasts between two and eight years before periods stop entirely — about four years on average (Womenshealth.gov). During those years, estradiol doesn't fall in a clean line. It oscillates, sometimes wildly, before declining for good. The hormonal signal that quieted hunger, kept fat in the hips and thighs, and protected skeletal muscle becomes unreliable.
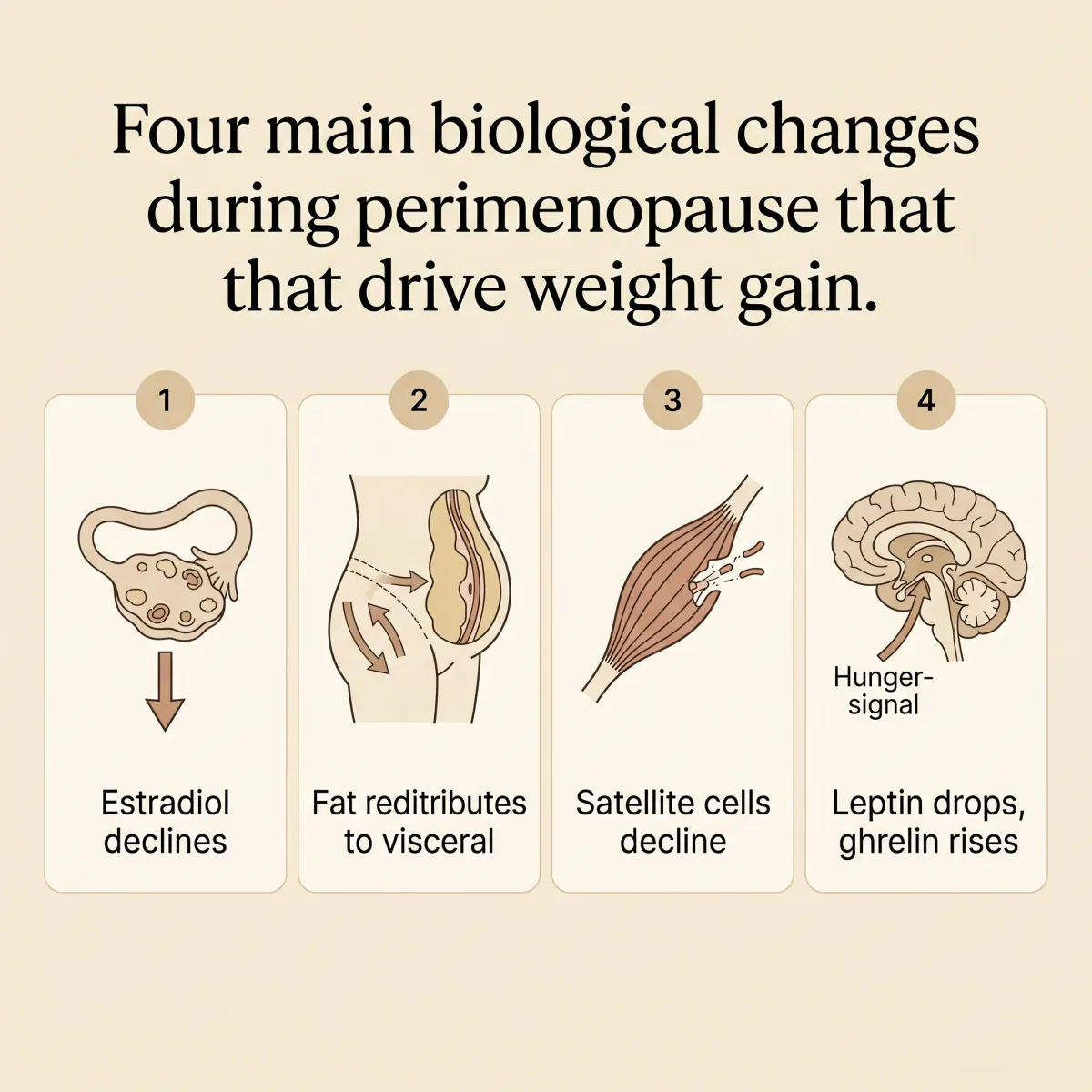
The four shifts that matter for weight
Fat redistribution is the first. With estradiol high, adipose tissue lands peripherally — hips, thighs, breasts. As it falls, the same calories deposit centrally. Jean Marino, a menopause specialist at University Hospitals, describes it directly: "There is a tendency for subcutaneous fat to convert to visceral fat" during the transition, with the deeper compartment carrying cardiovascular and metabolic risk independent of total body weight (University Hospitals). A 130-pound woman at 38 and a 130-pound woman at 53 can metabolize entirely differently.
Muscle is the second. Estradiol does more than run the cycle — it keeps muscle stem cells (satellite cells) responsive. A 2019 review of musculoskeletal aging found that "exercise-induced activation of satellite cells is less effective in the absence of estrogen," with hormone-therapy users showing measurably greater strength (Collins, Laakkonen & Lowe, 2019). The same workout doesn't build the same muscle at 53 as at 33.
Appetite regulation is the third. Perimenopausal sleep disruption, driven by night sweats, cuts leptin and raises ghrelin (University Hospitals). Women who reliably stopped at one slice now find themselves at two. The willpower frame misses the biology under it.
Thermogenesis is the fourth. Fernando Lizcano's 2022 Frontiers review analyzed the SWAN cohort and found women gain "2 to 3 kgs over the course of the menopausal transition" — driven more by menopause itself than by aging, partly through reduced resting thermogenesis (Lizcano, 2022).
Stack those four, and you have a population that responds differently to traditional weight-loss tools — and, surprisingly, sometimes better to peptides.
Do GLP-1 Peptides Even Work in Women Over 50? The SURMOUNT Data
Until 2025, the honest answer was "we think so, but the trials weren't designed to ask." Most phase-3 obesity trials enrolled mixed-age populations and reported pooled results. Whether a 52-year-old in active perimenopause responded the same as a 38-year-old wasn't a question the data structure could resolve cleanly.
That changed when Beverly Tchang, an endocrinologist at NewYork-Presbyterian and Weill Cornell, published a post-hoc analysis of 2,542 women across all three SURMOUNT tirzepatide trials, broken out by reproductive stage (Tchang et al., Obesity, 2025). The categories — premenopausal, perimenopausal, postmenopausal — followed the standard reproductive-aging framework rather than self-report.
The headline: tirzepatide produced a 26% body-weight reduction in premenopausal women, 23% in perimenopausal women, and 23% in postmenopausal women, against placebo losses of 2-3% in every group. Waist circumference dropped 20-22 cm with tirzepatide vs. 4-5 cm with placebo, again across all stages. Between 97% and 98% of women on the drug — premeno, peri, or postmeno — hit the conventional 5% weight-loss threshold; 69-73% hit 20% (Tchang et al., 2025).
The conclusion makes this analysis a clinical anchor: "Treatment effectiveness remained consistent irrespective of reproductive stage." Tchang told NewYork-Presbyterian: "Clinicians prescribing tirzepatide can feel more confident recommending this medication to their patients, especially women reporting menopause-related weight gain" (NewYork-Presbyterian Advances).
Semaglutide tells a similar story at lower doses
Joana Nicolau and colleagues at Hospital Universitari Son Llàtzer ran a 4-month low-dose semaglutide study (1 mg weekly), comparing premenopausal and postmenopausal women head to head. Postmenopausal women started heavier — 95 kg vs. 86 kg — but lost a comparable absolute amount, 5.9 kg vs. 4.5 kg (Nicolau et al., Metab Syndr Relat Disord, 2025). Fat- and lean-mass changes followed the same pattern in both groups.
The two studies converge on a single point worth saying directly: a 52-year-old considering Wegovy, Zepbound, Mounjaro, or compounded semaglutide is not getting a watered-down version of what younger participants got. Roughly the same chemistry, roughly the same outcome.
The HRT + Peptide Stack Mayo Clinic Just Quantified
If a peri- or postmenopausal woman is also a candidate for menopausal hormone therapy — typically estradiol with or without progesterone — pairing the two appears to amplify weight loss meaningfully beyond the peptide alone.

The cleanest evidence came from Mayo Clinic Jacksonville. Maria Hurtado-Andrade and colleagues had previously published a retrospective analysis of 106 postmenopausal women on semaglutide, finding that those also using hormone therapy lost 16 ± 6% of body weight at 12 months versus 12 ± 8% in non-users — about 30% greater weight loss, statistically significant at p=0.04 (Hurtado et al., Menopause, 2024). One drug, one center, but a strong enough signal to motivate a follow-up.
The follow-up arrived at ENDO 2025 in San Francisco. Regina Castaneda, a research fellow on the Mayo endocrinology team, presented an analogous retrospective cohort: 120 postmenopausal women on tirzepatide, 40 also on hormone therapy, followed for a median of 18 months. The combined arm lost 17% of body weight; tirzepatide alone, 14% (Endocrine Society press release).
The percentage difference understates the practical effect. Forty-five percent of the combination group hit the ≥20% weight-loss threshold — a level associated with bariatric-surgery-class metabolic improvement. Only 18% of the tirzepatide-only group did (Medical Update Online coverage). Castaneda summarized her finding plainly: "These data are the first to show the combined use of tirzepatide and menopause hormone therapy significantly increases treatment effectiveness."
The mechanism isn't pinned down. Reasonable hypotheses: estradiol restores some insulin sensitivity, which the GLP-1/GIP pathway leverages more efficiently; estradiol reduces visceral fat preferentially while tirzepatide reduces total fat, so the two compound in different compartments; or estradiol attenuates the lean-mass loss that often accompanies fast weight loss, leaving a higher metabolic rate to keep working with. Castaneda stopped short of a mechanistic claim: "Achieving these outcomes with a second obesity medication may indicate a broader efficacy trend for pairing these two classes of medications."
Two cautions before reading this as prescriptive. Both Mayo studies are observational — retrospective cohorts, not RCTs. Selection bias is real: women on HRT may be more health-engaged, more affluent, more likely to also exercise. Authors adjusted for baseline weight, age, diabetes status, and behavioral support, and the effect held. A randomized trial would be more definitive. Second, HRT isn't appropriate for every woman — personal and family history of breast cancer, blood-clotting disorders, certain cardiovascular conditions all change the calculus. The combo is a conversation with a clinician who knows your full history, not a default.
Side Effects That Look Different on a 52-Year-Old Body
The published GLP-1 side-effect lists were assembled mostly from younger trial populations. They're accurate, but they don't always capture how the same drug presents in a body already navigating perimenopause.
Hair shedding is one. The FDA label and Penn Medicine's analysis of post-marketing reports both note hair loss as a Zepbound side effect — 7.1% in women versus 0.5% in men, a roughly fourteenfold gap (Penn Medicine analysis cited via Gift From Within). Most cases begin around month three, peak at months four to six, and resolve in roughly 85% of women by month twelve. The pattern is consistent with telogen effluvium — the same temporary shedding triggered by sudden caloric deficits, postpartum, or major surgery. For a woman already noticing perimenopausal thinning at the temples and crown, the effect can read as "the drug is destroying my hair" when the more accurate framing is "rapid weight loss has accelerated a process that was already underway." Adequate protein and ferritin labs help.

Dehydration is the second pattern. Mary Claire Haver, a menopause specialist focused on the over-50 cohort, has flagged it directly: "GLP-1s also reduce thirst signals, which compounds the risk in menopausal women already prone to lower hydration" (via Gift From Within). Estradiol decline already affects fluid balance; a drug that quiets thirst can produce headaches, lightheadedness, and constipation that gets blamed on the drug's GI effects when the upstream issue is simply low water intake.
Constipation lands harder in the postmenopausal gut. Slowed gastric emptying — the same mechanism that creates fullness — interacts with the slower colonic transit common after 50. Magnesium glycinate or citrate at bedtime, plus 80-100 oz of water daily, is the standard mitigation.
Menstrual changes show up in roughly 4% of women on Zepbound per Penn Medicine post-marketing reports — but in perimenopausal women whose cycles are already irregular, attribution is genuinely difficult. The honest position is "we don't know how often the drug is doing it versus the transition." Same for mood: both perimenopause and rapid caloric restriction can produce irritability, fatigue, and low mood; teasing apart drug from biology requires patience and good baseline tracking.
One real safety overlay: GLP-1s carry rare but documented risk of pancreatitis and gallbladder disease, somewhat elevated in women, in older patients, and in those losing weight rapidly — all three describe the over-50 woman starting therapy. Persistent severe abdominal pain on these drugs is never a "wait and see" symptom.
Muscle, Bone, and Why You Cannot Skip Resistance Training
The lean-mass concern is the criticism of GLP-1 weight loss that legitimately gets sharper after 50. Without specific intervention, roughly 25-40% of total weight lost on these drugs comes from lean tissue rather than fat. In a 30-year-old, that's recoverable with protein and lifting. In a 55-year-old already dealing with reduced satellite-cell function and dropping bone density, the same percentage can mean accelerating an underlying sarcopenia trajectory.

The Collins, Laakkonen, and Lowe review made the point clinically: estrogen is essential for satellite cell maintenance, and the muscle response to a strength stimulus is "less effective in the absence of estrogen" (Collins et al., 2019). Strength training still works — it just has to be deliberate, consistent, and built around progressive overload, not the casual once-a-week class that may have been enough at 35.
The clinical recommendations from physicians who treat this population converge on a similar floor. Jolene Brighten, a board-certified naturopathic endocrinologist, recommends 1.2-1.6 g of protein per kg per day, distributed across meals, with resistance training "2-3 times weekly minimum, targeting major muscle groups" — and is direct: "GLP-1 without strength training is a bad idea" (Brighten podcast). Mary Claire Haver pushes the protein floor higher for menopausal women specifically, 1.5-1.8 g/kg, on the grounds that the satellite-cell response is already attenuated and needs more substrate (via Gift From Within).
For a 70-kg (154-lb) woman, 1.5 g/kg is about 105 g of protein per day. Across three meals plus a snack, that's 25-35 g per occasion — a six-ounce salmon fillet, a cup of cottage cheese, a four-egg omelet, a chicken breast. The leucine threshold (the amino acid that triggers muscle protein synthesis) is roughly 2.5-3 g per meal, which most of these portions hit comfortably. Skipping protein at breakfast — common when GLP-1 appetite suppression makes coffee feel like enough — is the most common failure mode, and it costs a daily synthesis cycle.
Bone is the parallel concern. Estradiol decline accelerates resorption, which is why DEXA-scan baseline data become useful before starting any peptide that produces fast weight loss. Weight loss + low estrogen + inadequate weight-bearing exercise is the textbook recipe for osteoporotic fracture risk to climb. Resistance training is not optional here — it's the single intervention that protects bone, muscle, and the metabolic rate that keeps weight off after the drug is reduced or stopped.
A Sensible Protocol If You Are Starting at 48 or 55
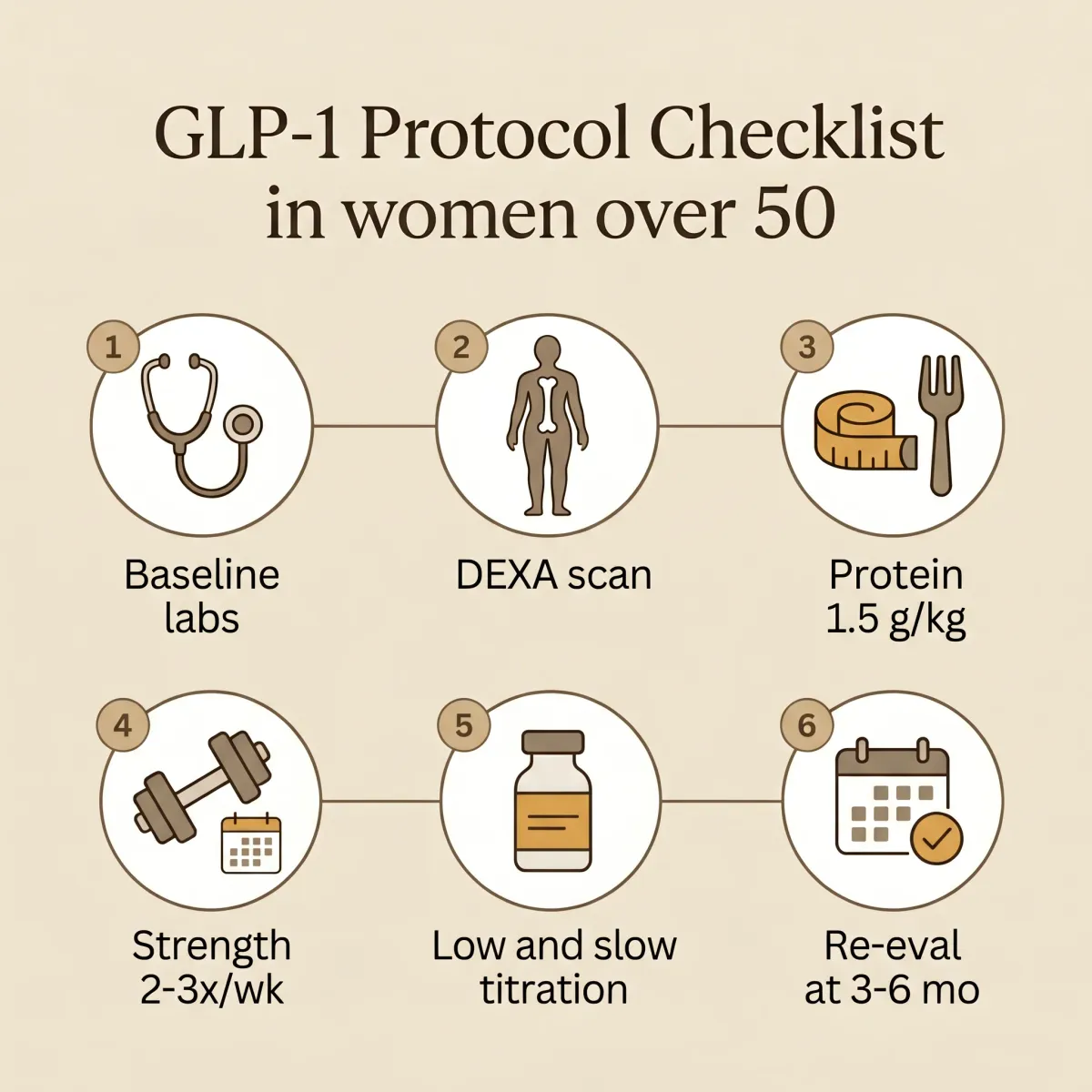
The clinicians treating this population have converged on a roughly common pre-treatment workup. Not regulatory, but every detail in it has a reason.
Before the first injection
Brighten's pre-treatment lab list, which echoes the workup at most established peptide clinics, includes fasting insulin, HbA1c, full lipid panel, hs-CRP, comprehensive metabolic panel with liver enzymes, full thyroid panel (TSH, free T4, free T3, TPO), and sex hormones — total and free testosterone, SHBG, DHEA-S, plus FSH and estradiol when menopausal status is unclear. Body composition via InBody or DEXA establishes a baseline for lean mass and bone density (Brighten podcast). The point isn't completeness — it's that these data determine whether the right next step is a peptide alone, peptide plus HRT, lifestyle-first, or referral.
Dosing slower than the manufacturer's schedule
Lilly's tirzepatide titration steps up every four weeks: 2.5, 5, 7.5, 10, 12.5, 15 mg. The schedule was designed for trial efficiency. In clinical practice, women over 50 often do better with eight-week steps and a willingness to stay at the lowest therapeutic dose still producing change. Brighten emphasizes that "escalation is not mandatory" and many patients stay therapeutic on starting doses (Brighten podcast). A 10 mg dose that triggers severe nausea isn't delivering more efficacy than the 7.5 mg that was working.
The HRT conversation
If a woman is already a candidate for menopausal hormone therapy on symptom grounds — meaningful hot flashes, sleep disruption, vaginal symptoms, mood changes — the Mayo data suggest the metabolic case becomes additive rather than competing. Transdermal estradiol carries lower thrombotic risk than oral; serum estradiol levels in the 60-100 pg/mL range are typical therapeutic targets, though individual goals vary (Brighten podcast). For women with intact uteri, progesterone protects the endometrium. None of this is a self-prescription — but it's a conversation worth having with a menopause-trained clinician before starting a peptide alone if eligibility is on the table.
Lifestyle, not as decoration
Strength training 2-3 days a week, protein 1.5-1.8 g/kg, 80-100 oz of water, magnesium at bedtime, eight hours of sleep, and continued treatment of perimenopause symptoms separately from the weight question. The peptide handles appetite and glucose. The HRT (if appropriate) handles the metabolic background. The lifestyle work protects the body composition that keeps the loss durable.
Re-evaluation at three to six months
Repeat the body-composition scan, the metabolic panel, the symptom inventory. Decide whether to hold the dose, increase, or — if results exceed goals — taper. A 23% body weight reduction in a woman who started at 180 lb is 41 lb. Any peptide therapy is meant to be revisited, not autopiloted; the SURMOUNT-4 data suggest the effect persists primarily while the drug is on board, which makes the long-term plan a clinical conversation in itself.
Frequently Asked Questions
Will GLP-1 peptides work as well for me at 53 as they would have at 33?
Per the Tchang post-hoc analysis of the SURMOUNT trials, essentially yes for tirzepatide — premenopausal women lost 26%, perimenopausal and postmenopausal women lost 23%. The gap was small enough that researchers concluded effectiveness was "consistent irrespective of reproductive stage" (Tchang et al., Obesity 2025). Semaglutide data from Nicolau and colleagues show a similar pattern at lower doses.
If I'm already on hormone therapy, does that change anything?
The Mayo Clinic retrospective data say yes — favorably. Hurtado's 2024 study showed semaglutide users on HRT lost 16% versus 12% without it at one year. Castaneda's 2025 follow-up showed tirzepatide users on HRT lost 17% vs. 14% and were 2.5 times more likely to hit ≥20% loss. Observational, not randomized — but the signal has now appeared across two different drugs in the same patient population (Castaneda et al., ENDO 2025).
I lost weight on Mounjaro but my hair started shedding at month four. Is that the drug?
Most likely a combination. Hair shedding rates on Zepbound are 7.1% in women vs. 0.5% in men, with onset typically at month three and resolution by month twelve in roughly 85% of cases. The pattern is consistent with telogen effluvium triggered by rapid weight loss, which a perimenopausal hormonal window can amplify. Adequate protein (1.5 g/kg minimum) and ferritin above 70 ng/mL are the standard mitigations (per Penn Medicine post-marketing data).
How much protein do I really need?
For weight loss on a GLP-1 in the over-50 cohort, Mary Claire Haver recommends 1.5-1.8 g/kg/day; Brighten's floor is 1.2-1.6 g/kg. For a 154-lb woman, that's roughly 105-126 g daily, distributed across at least three meals to hit the leucine threshold for muscle protein synthesis at each one (Brighten podcast).
Can I do this without strength training?
You can lose weight on the scale without it, but the lean-mass loss in a postmenopausal body is harder to recover than in a younger one because estradiol's role in satellite cell maintenance is already attenuated. The clinical consensus is that resistance training 2-3 times per week is non-negotiable, not optional decoration around the peptide (Collins et al., 2019).
Related Articles
- The Stubborn Belly Fat Peptide: Why Tesamorelin Is Going Viral with Women Over 40
- Why Tirzepatide Users Lose 22% of Their Body Weight — and What Happens When They Stop
- Tirzepatide vs. Semaglutide: Which GLP-1 Peptide Actually Melts More Fat?
- The GLP-1 Side Effect List Your Doctor Probably Won't Mention
- How Long Should You Stay on Weight Loss Peptides? The Answer Is Not "Forever"
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











