You probably know vitamin K as the one involved in blood clotting. And you might eat your leafy greens thinking you have it covered. But there is a second form of this nutrient, vitamin K2, that most people have never heard of, and it does something entirely different in your body. Instead of working in the liver to manage clotting factors, K2 operates in your bones and blood vessels, influencing where calcium ends up and whether it strengthens your skeleton or hardens your arteries.
An estimated 31% of the general population has functional vitamin K insufficiency, meaning their bodies cannot fully activate the proteins that keep calcium in check. And because K2 deficiency does not cause obvious symptoms the way scurvy or rickets would, it often goes undetected for years while calcification quietly accumulates. Here is what the research actually says about K2, and whether you should be paying attention to it.
What Makes Vitamin K2 Different From K1?
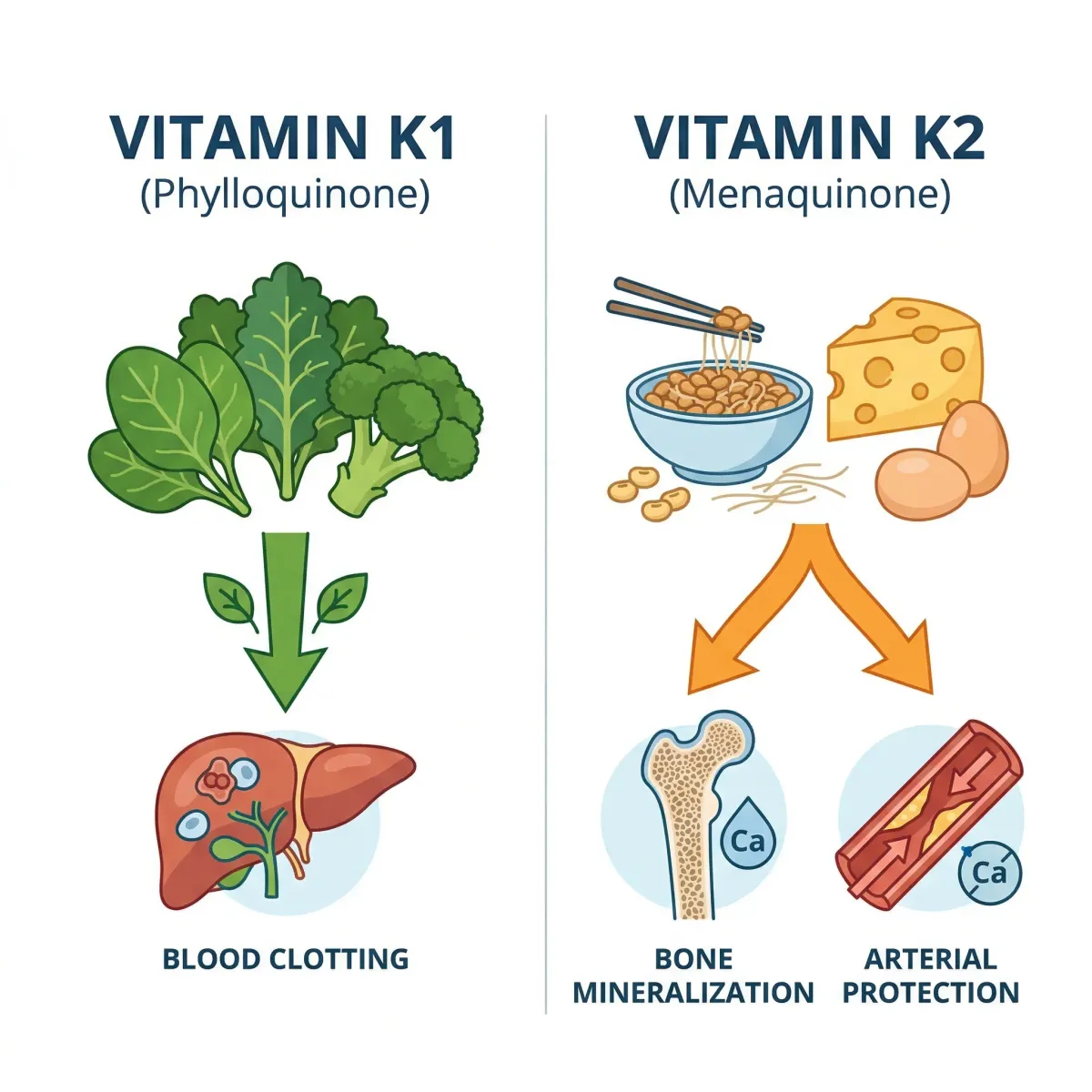
Vitamin K is not a single compound but a family of molecules sharing a common chemical backbone. The two natural forms, K1 (phylloquinone) and K2 (menaquinones), look similar on paper but behave very differently once they enter your bloodstream.
Vitamin K1 concentrates almost exclusively in the liver, where it drives the production of clotting factors that stop bleeding. You get it from spinach, kale, broccoli, and other green vegetables. For most healthy adults eating a varied diet, K1 intake is rarely an issue.
Vitamin K2, on the other hand, bypasses the liver and distributes to extrahepatic tissues, particularly bones and arterial walls. According to the NIH Office of Dietary Supplements, long-chain menaquinones like MK-7 are transported more efficiently to these tissues. Think of K1 as the local branch manager handling clotting, while K2 is the field agent working in the bones and blood vessels where calcium regulation actually matters for long-term health.
K2 itself comes in several subtypes, designated by the length of their molecular side chains. MK-4 (four isoprene units) and MK-7 (seven units) are the two forms you will encounter most often in supplements and research literature. The differences between them matter when choosing a supplement, and we will break that down later.
How Vitamin K2 Directs Calcium to the Right Places
Calcium is essential for strong bones, but it becomes dangerous when it deposits in soft tissues like arteries and heart valves. Your body has a built-in system for keeping calcium where it belongs, and vitamin K2 runs it.
The key player is a protein called matrix Gla protein, or MGP. Synthesized primarily by cells in your blood vessel walls, MGP is considered the strongest inhibitor of vascular calcification that researchers have identified. But here is the catch: MGP is produced in an inactive form. It requires vitamin K2 as a cofactor to undergo a chemical modification called gamma-carboxylation, which essentially switches it on.
When K2 is abundant, MGP gets fully activated and performs several protective functions. It directly inhibits the formation and growth of calcium crystals in artery walls. It blocks a protein called BMP-2 that would otherwise reprogram smooth muscle cells into bone-like cells capable of depositing calcium. And it works alongside other calcification inhibitors like fetuin-A to keep the arterial environment hostile to mineral buildup.
On the bone side, K2 activates a separate protein called osteocalcin, sometimes called bone Gla protein. Once carboxylated by K2, osteocalcin helps bind calcium into the bone matrix during mineralization. So K2 effectively operates a two-way traffic system: it pushes calcium into bones while simultaneously preventing it from settling in arteries.
The calcium paradox in brief: Without adequate K2, you can have weak bones AND calcified arteries at the same time, because the proteins that direct calcium to the right destination are sitting idle in their inactive forms.
This dual mechanism helps explain a pattern that puzzled researchers for years. Many older adults, particularly postmenopausal women, develop both osteoporosis and arterial calcification simultaneously. The same K2 deficiency that leaves osteocalcin unable to build bone also leaves MGP unable to protect arteries. Fixing K2 status might improve both problems at once, though clinical trials are still working to confirm that.
The Evidence Behind Vitamin K2 and Stronger Bones
Researchers have been studying vitamin K and bone health for decades. The findings are real, but they come with important fine print.
A 2006 systematic review and meta-analysis by Cockayne and colleagues examined 13 randomized controlled trials, most conducted in Japan with postmenopausal women. The results were striking: MK-4 supplementation significantly reduced rates of hip fractures, vertebral fractures, and all nonvertebral fractures. These trials predominantly used pharmacological doses of MK-4 at 45 mg per day, far exceeding what you would get from diet alone.
A subsequent trial found that the more commonly available MK-7 form also delivered meaningful bone benefits at much lower doses. In postmenopausal women, 180 mcg of MK-7 daily for three years improved bone strength and decreased the loss in vertebral height in the lower thoracic region. That is a dose easily achieved through supplementation or a diet rich in fermented foods.
However, the picture is not entirely uniform. Other randomized clinical trials, particularly those conducted in Western populations already receiving adequate calcium and vitamin D, found that vitamin K supplementation had no significant effect on bone mineral density in elderly men or women. One explanation involves vitamin D status, which itself influences calcium absorption and bone metabolism. When both vitamin D and calcium are already optimized, the additional benefit of K2 may be harder to detect.
| Study / Form | Dose | Duration | Key Finding |
|---|---|---|---|
| Cockayne meta-analysis (MK-4) | 45 mg/day | 6-36 months | Reduced hip, vertebral, and nonvertebral fractures |
| Knapen et al. (MK-7) | 180 mcg/day | 3 years | Improved bone strength, decreased vertebral height loss |
| Binkley et al. (MK-4 + K1) | 45 mg MK-4 / 1 mg K1 | 12 months | Reduced undercarboxylated osteocalcin, but no BMD change |
In Japan, a pharmacological dose of 45 mg MK-4 has been approved as a treatment for osteoporosis. The European Food Safety Authority has also recognized a cause-and-effect relationship between vitamin K intake and maintenance of normal bone. The FDA in the United States has not yet authorized a comparable health claim, though this reflects regulatory process differences rather than a fundamental disagreement about the science.
Can Vitamin K2 Actually Protect Your Arteries?
The heart health case for vitamin K2 rests on two types of evidence: big population studies that tracked what people ate for years, and clinical trials where researchers gave people K2 supplements and measured what happened.
The landmark Rotterdam Study followed 4,807 Dutch subjects with no prior heart attack history for an average of seven years. The findings were notable: participants in the upper tertials of dietary K2 intake had a 57% lower risk of coronary heart disease mortality (RR=0.43) and a 26% reduction in all-cause mortality (RR=0.74) compared to those with the lowest intake. Vitamin K1, despite being consumed in larger amounts, showed no association with cardiovascular outcomes at all.
A Norwegian prospective study spanning 11 years replicated this pattern, finding a 48% lower coronary artery disease risk (HR=0.52) among those with higher K2 intake. And in a large Japanese cohort of nearly 30,000 participants followed for 16 years, intake of natto, the richest dietary source of MK-7, was linked to a 25% lower cardiovascular mortality risk.
On the intervention side, the evidence is more mixed but still encouraging. A three-year randomized controlled trial found that MK-7 supplementation at 180 mcg per day significantly reduced arterial stiffness in healthy postmenopausal women, as measured by pulse wave velocity. Multiple other trials have demonstrated that K2 supplementation produces a dose-dependent reduction in circulating dp-ucMGP, the biomarker that reflects vitamin K deficiency and predicts cardiovascular risk.
A recent meta-analysis pooling prospective data found that elevated dp-ucMGP, signaling poor vitamin K status, was associated with an 84% higher risk of all-cause mortality (pooled HR=1.84) and a 96% higher risk of cardiovascular mortality (pooled HR=1.96).
Where the evidence gets more complicated is with calcification scores. Several short-term trials, particularly in patients on hemodialysis, have failed to show a significant reduction in existing arterial calcification despite improving K2 biomarkers. Researchers note that these studies may have been too short (6-18 months) and too small to capture what is likely a very slow process of calcification reversal. The question is not whether K2 influences calcification biology, which the MGP mechanism makes clear, but whether supplementation over practical timeframes can measurably reverse damage that has accumulated over decades.
The cardiovascular case for K2 is strongest in prevention: maintaining adequate K2 status throughout life appears to slow the rate at which arteries stiffen and calcify. Whether K2 supplementation can reverse existing calcification remains an open and actively researched question, with several ongoing clinical trials expected to report in coming years.
MK-4 vs. MK-7: Which Form Should You Take?
If you have looked at vitamin K2 supplements, you have noticed two primary options: MK-4 and MK-7. They are both vitamin K2, but they behave very differently in your body.
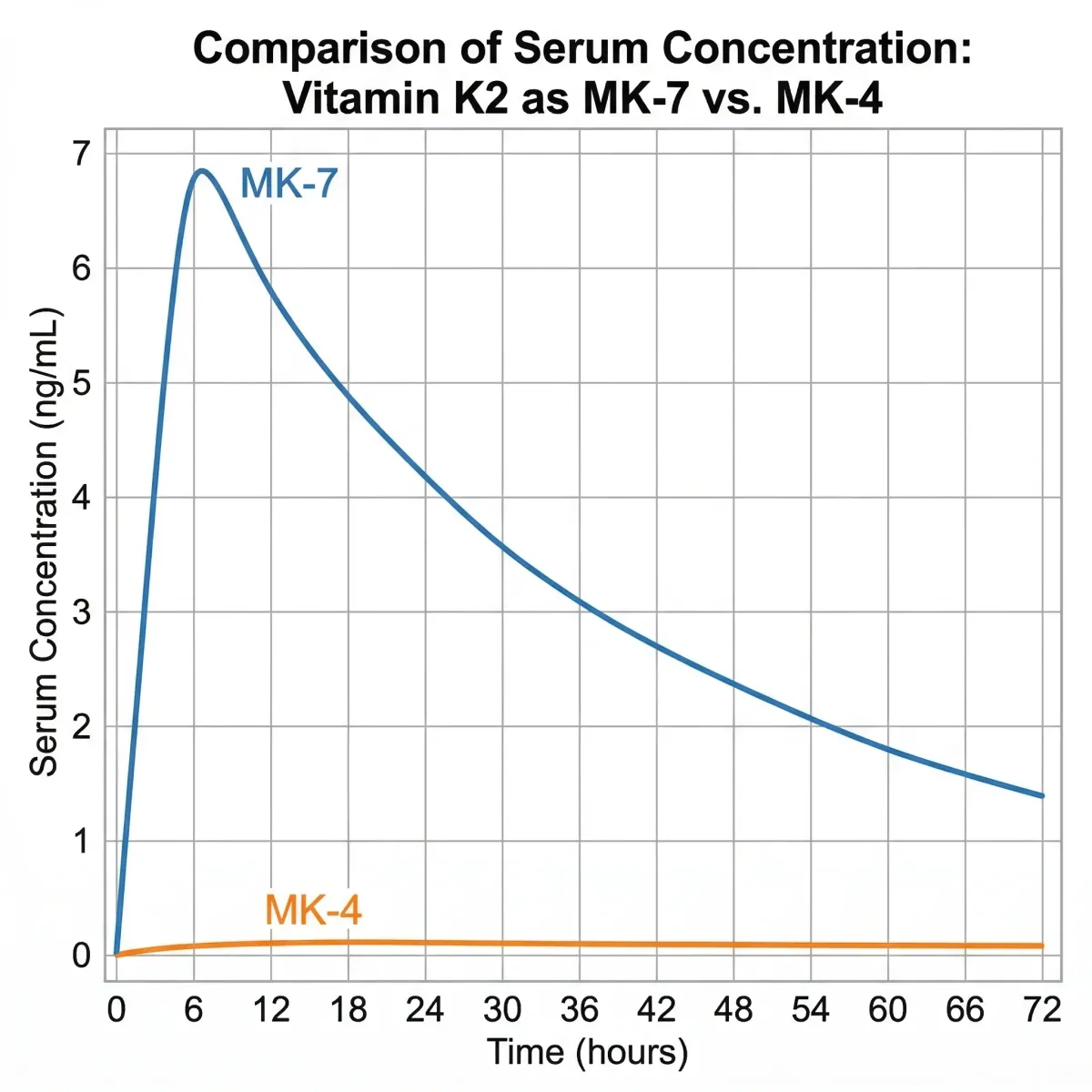
A bioavailability study in healthy Japanese women revealed a startling finding: when given a single 420 mcg dose, MK-4 was not detectable in the serum of any subject at any time point. MK-7, given at the same dose, was well absorbed, reached peak blood levels at six hours, and remained detectable for up to 48 hours. When the study extended to seven days of daily dosing at 60 mcg, MK-4 still failed to raise blood levels, while MK-7 produced significant and consistent increases.
| Property | MK-4 | MK-7 |
|---|---|---|
| Bioavailability at nutritional doses | Very poor (undetectable in serum) | High (detectable 48+ hours) |
| Serum half-life | 1-2 hours | ~72 hours |
| Effective dose for osteocalcin activation | 1,500+ mcg/day | 45-90 mcg/day |
| Pharmacological dose (Japan, osteoporosis) | 45 mg/day | Not used at pharmacological doses |
| Main dietary sources | Eggs, meat, liver | Natto, some cheeses |
| Carboxylation of extrahepatic proteins | Requires high doses | Effective at nutritional doses |
This does not mean MK-4 is useless. At the pharmacological dose of 45 mg used in Japanese osteoporosis treatment, MK-4 clearly delivers fracture-reducing benefits. The body also converts all forms of vitamin K into MK-4 in certain tissues. Intriguingly, MK-7 supplementation actually increases MK-4 levels in extrahepatic tissues more effectively than MK-4 supplementation itself, suggesting MK-7 serves as a better delivery vehicle even for MK-4's tissue-specific functions.
For the cardiovascular benefits specifically, the evidence favors MK-7. The effective dose range of 180-360 mcg per day for cardiovascular improvements is well within what a single supplement capsule delivers. MK-7 also does not require the massive doses that MK-4 needs to achieve similar effects on vitamin K-dependent protein activation.
Where to Find Vitamin K2 in Your Diet
Getting enough K2 through Western diets alone is genuinely difficult, which partly explains why deficiency is so widespread. Unlike K1, which is abundant in any salad, K2 hides in a narrow range of foods that many people rarely eat.
The undisputed champion is natto, a Japanese fermented soybean dish that delivers approximately 850 mcg of MK-7 per three-ounce serving, which is over 700% of the daily value for vitamin K. Three ounces of natto provides more K2 than most people consume in a month. The problem, of course, is that natto has a strong, ammonia-like flavor and sticky, stringy texture that many people outside of Japan find unappealing.
| Food Source | K2 Form | Approximate K2 Content |
|---|---|---|
| Natto (3 oz) | MK-7 | 850 mcg |
| Hard cheeses (Gouda, 1.5 oz) | MK-4, MK-8, MK-9 | 20-50 mcg |
| Chicken breast (3 oz) | MK-4 | 13 mcg |
| Egg yolk (1 large) | MK-4 | 4 mcg |
| Ground beef (3 oz) | MK-4 | 6 mcg |
| Chicken liver (3 oz) | MK-4 | 6 mcg |
| Cheddar cheese (1.5 oz) | MK-4 | 4 mcg |
If natto is not on your menu, the next best dietary sources are certain fermented cheeses, particularly Gouda, Brie, and Edam, which contain modest amounts of various menaquinones produced during bacterial fermentation. Animal products like eggs, chicken, and organ meats contain MK-4 but in small quantities. A diet emphasizing these foods alongside polyphenol-rich whole foods can contribute to overall cardiovascular protection, though the K2 from meat and dairy alone is unlikely to reach the 180-360 mcg range associated with cardiovascular benefits in clinical studies.
It is worth noting that the Adequate Intake for total vitamin K, set at 120 mcg for adult males and 90 mcg for adult females, was established primarily with blood clotting in mind and does not differentiate between K1 and K2. The amounts needed for optimal bone and cardiovascular protection through K2-dependent proteins may be higher than what this guideline reflects, and current recommended intakes primarily address K1 from vegetables.
Myths vs. Facts About Vitamin K2
| Myth | Fact |
|---|---|
| Eating leafy greens gives you enough K2 | Leafy greens provide K1, not K2. These are different vitamers with different functions and tissue distribution. K1 stays in the liver; K2 goes to bones and arteries. |
| Vitamin K supplements are dangerous because they affect blood clotting | K2 at nutritional doses (90-360 mcg) does not cause a hypercoagulable state. The WHO has set no upper tolerance level for vitamin K due to its low toxicity potential. However, people on warfarin must consult their doctor. |
| All K2 supplements are the same | MK-4 and MK-7 have dramatically different bioavailability. MK-4 at nutritional doses does not even reach detectable serum levels, while MK-7 is absorbed efficiently and remains active for days. |
| Calcium supplements alone are enough for bone health | Calcium without adequate K2 and vitamin D may actually increase cardiovascular risk by depositing calcium in arteries instead of bones. K2 activates the proteins that direct calcium to the right places. |
| K2 can reverse existing arterial calcification | Animal studies show potential for reversal, but human trials have not yet demonstrated significant reversal of established calcification. K2's strongest evidence is in prevention and slowing progression. |
| You can get enough K2 from gut bacteria | While gut bacteria produce menaquinones, it is unclear how much of this is actually absorbed. Research suggests it contributes partially but likely not enough to optimize extrahepatic K-dependent protein function. |
Frequently Asked Questions
How much vitamin K2 should I take daily?
For general bone and cardiovascular support, clinical research suggests 90-180 mcg of MK-7 per day. The studies demonstrating reduced arterial stiffness used 180 mcg daily, while those showing bone benefits used 180 mcg MK-7 or the much higher pharmacological dose of 45 mg MK-4. If you are supplementing primarily for heart health, 180-360 mcg of MK-7 is the range most supported by evidence. Always discuss supplementation with your healthcare provider, especially if you take blood-thinning medications.
Can I take vitamin K2 if I am on blood thinners?
If you take warfarin (Coumadin) or similar vitamin K antagonists, you must talk to your doctor before taking K2 supplements. Warfarin works by blocking vitamin K activity, so adding K2 could reduce the drug's effectiveness and increase clotting risk. This interaction does not apply to newer anticoagulants like rivaroxaban or apixaban, which work through a different mechanism. In fact, some research suggests that patients switching from warfarin to these newer agents may benefit from improved vitamin K status.
Should I take vitamin K2 with vitamin D3?
There is a logical rationale for pairing them. Vitamin D3 increases calcium absorption from the gut and stimulates osteocalcin production, while K2 activates osteocalcin so it can actually bind that calcium into bone. Without K2, the increased calcium from D3 supplementation theoretically has fewer places to go, which could contribute to soft tissue calcification. While clinical trials specifically testing the D3+K2 combination are still limited, the mechanistic logic is sound enough that many practitioners recommend them together.
Is vitamin K2 safe during pregnancy?
The Adequate Intake for vitamin K during pregnancy is 90 mcg, the same as for non-pregnant adult women. There are no documented cases of vitamin K toxicity at any dose, and the Food and Nutrition Board did not establish an Upper Limit for vitamin K because of its low potential for harm. That said, pregnant women should discuss any supplementation with their healthcare provider, as limited research exists specifically on K2 supplementation during pregnancy.
How long does it take for vitamin K2 to work?
Biomarker improvements, specifically reductions in uncarboxylated osteocalcin and dp-ucMGP, can be measured within weeks of starting supplementation. However, the downstream effects on bone density and arterial stiffness take much longer. The clinical trials showing bone benefits ran for one to three years, and the cardiovascular stiffness improvements in postmenopausal women were measured after three years of daily MK-7. This is a slow-burn nutrient, not a quick fix.
Related Articles
- Vitamin K2 and Arterial Calcification: Can This Overlooked Vitamin Protect Your Arteries? — A deeper look at K2's role in preventing and potentially reversing arterial calcification.
- The Best Types of Magnesium for Heart Health — Another mineral that plays a critical role in cardiovascular and bone health, often deficient alongside K2.
- Vitamin D3 and Second Heart Attack Prevention — The synergistic partner to K2, and why taking D3 without K2 may miss part of the picture.
- Polyphenol-Rich Foods for Heart Health — Dietary compounds that complement K2's cardiovascular protective mechanisms.
- Collagen Supplements for Skin, Joints, and Gut — Understanding the structural proteins that work alongside calcium and K2 in maintaining skeletal integrity.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.