
The conversation does not happen on a podium. It happens at mile twenty of a long Sunday run, one stranger asking another, "have you tried the peptide thing yet." The list that follows is short and almost always the same: BPC-157 for an angry Achilles, TB-500 for a quad that will not stop seizing, MOTS-c because someone on a podcast said it doubled treadmill capacity in old mice. Telehealth clinics write the prescriptions. The local 50K is a different race than it was three years ago.
Here is what the science actually says. Almost every peptide on that list is on the World Anti-Doping Agency Prohibited List for in- and out-of-competition use. Almost none have a single completed phase III human trial. The one that does, collagen, is the one nobody whispers about, because it sits in a 30-dollar tub at the supermarket. This guide walks the evidence, names the regulators, and is direct about which compounds have human data and which have a stack of rodent studies and an Instagram budget.
Why Endurance Athletes Are Looking at Peptides
Marathoners stress connective tissue near-daily. Tendon, ligament, fascia, and the small stabilizers nobody trains directly all take a cumulative beating no rest week fully reverses. Sleep, NSAIDs, and the occasional cortisone shot manage symptoms. Peptides are sold as something different: short signaling molecules that instruct cells to rebuild specific tissues rather than dampen pain.
That framing is partly accurate. Peptides are short amino-acid chains that bind specific receptors and trigger downstream signaling: collagen synthesis, angiogenesis, AMPK activation, fibroblast migration. The framing is also where marketing starts to outrun the data. Most compounds being sold to recreational marathoners have been validated in rodents, dogs, or rabbits. Google search volume for BPC-157 and MOTS-c hit all-time highs in mid-2024, with 50 million tagged TikTok and YouTube views, while randomized human trials sit in the single digits. Telehealth clinics, longevity practices, and gray-market vendors have all caught up to the demand.
BPC-157: The Tendon Peptide Runners Whisper About
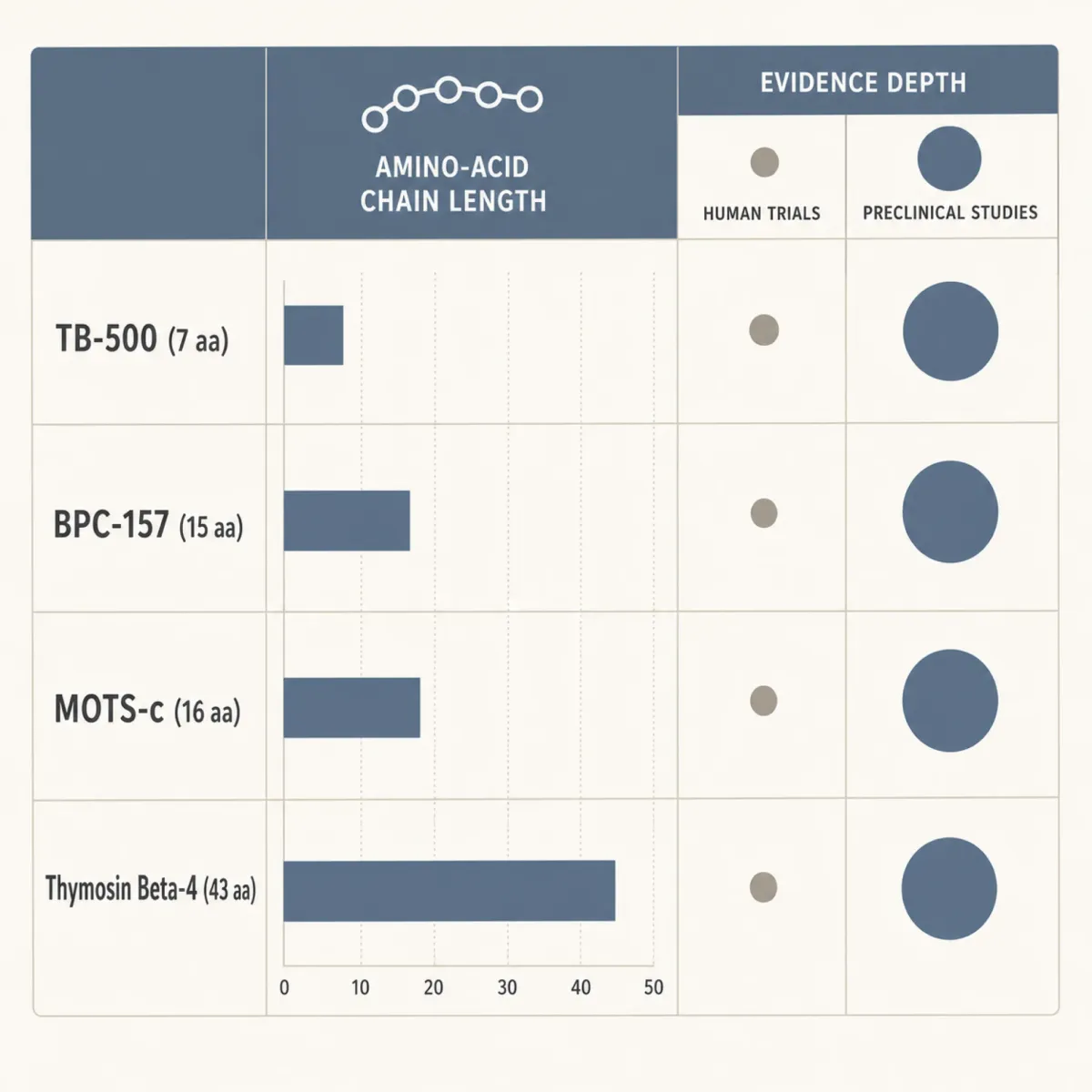
BPC-157, which stands for Body Protection Compound 157, is a synthetic 15-amino-acid sequence derived from a fragment of a protective protein originally isolated from human gastric juice by Dr. Predrag Sikiric in 1993. The animal data is genuinely striking. In Achilles tendon transection models, BPC-157 accelerates granulation, improves collagen organization, and protects local endothelium. The mechanism is plausible: VEGFR2 activation, Akt-eNOS-driven nitric oxide synthesis, ERK1/2 signaling for endothelial proliferation, and a macrophage shift from pro-inflammatory M1 toward reparative M2. For tendons, which are notoriously poorly vascularized, that angiogenic effect is what catches a runner's eye.
Here is the part that does not catch the eye. A 2025 narrative review in PMC and a 2025 systematic review in the HSS Journal by Vasireddi, Hahamyan, Salata, and colleagues both reach the same conclusion: of the 36 BPC-157 studies that survive a structured search across six databases, 35 are preclinical animal work and exactly one is human. That one is a retrospective case series of 12 patients receiving intra-articular injections for knee pain, with no control group. There are zero randomized controlled trials. The dosing protocols circulating online (250 micrograms twice daily, 500 mcg subcutaneous near the injury site) were extrapolated from rat studies, not validated in people. BPC-157 also has a circulating half-life of less than 30 minutes, meaning twice-daily protocols do not maintain steady plasma levels the way chronic antibiotics or hormones do.
WADA banned BPC-157 in 2022 under the S0 Unapproved Substances category, in- and out-of-competition. In January 2025, the FDA reclassified BPC-157 as a Category 2 Bulk Drug Substance, citing safety concerns and absence of human data. That move removed BPC-157 from the FDA Interim 503A Bulks List and effectively cut off compounding-pharmacy production. We covered the downstream consequences in our piece on the FDA reversal and what doctors are doing about it, with a deeper dose-and-research breakdown in our earlier BPC-157 evidence and dosage guide.
TB-500 and Thymosin Beta-4: Recovery From High Volume
The naming is genuinely confusing. Thymosin Beta-4 is the natural 43-amino-acid peptide produced by the thymus, involved in actin regulation and cell migration. TB-500 is a synthetic 7-amino-acid fragment (Ac-LKKTETQ) engineered from TB4's active site. They are not the same molecule, though most clinics treat them as such.
The 42% number you see everywhere on the internet comes from Malinda et al. in the Journal of Investigative Dermatology (1999). In a rat full-thickness wound model, topical or intraperitoneal Tβ4 increased re-epithelialization by 42% over saline at day 4 and 61% at day 7, with wound contraction at least 11% higher than controls. Cell migration jumped 2- to 3-fold with as little as 10 picograms of peptide. The one human signal worth citing is cardiac, not athletic: a STEMI trial of TB4-pretreated endothelial progenitor cells reported a 37.5-meter gain in 6-minute walking distance at six months. The dose, delivery, and patient population are nothing like an injured marathoner self-injecting a vial labeled TB-500. There are no published human athletic-performance trials.
Maryke Louw, a chartered physiotherapist with a master's in sports injury management, makes the direct point: TB-500 was originally a horse-doping agent. "We're not horses. We don't know whether it is safe to use in humans nor do we know the long-term effect it might have on your health." The cancer concern is not theoretical hand-waving. Thymosin beta-4 is upregulated in many metastatic cancers and facilitates tumor-cell migration, and animal experiments show TB-500 accelerates dormant tumor growth and disrupts immune response. WADA prohibits TB-500 under S2 at all times. The Essendon Football Club saga ended with 32 players receiving two-year CAS bans over thymosin beta-4 in a team supplementation program. For the BPC-157-plus-TB-500 "Wolverine stack" you'll see promoted on athlete forums, we have a separate breakdown of the actual evidence; same problem at twice the dose.
AOD-9604: Fat Oxidation for Long Efforts
AOD-9604 is the one peptide in this guide with a substantive human safety dataset. It is the synthetic C-terminal fragment of human growth hormone (amino acids 177 to 191), engineered to retain the lipolytic effect without driving IGF-1 elevation or the carbohydrate-metabolism interference of full hGH. The original developer, Metabolic Pharmaceuticals, ran six clinical trials totaling roughly 900 subjects. None of those showed a drug-related serious adverse event or an IGF-1 signal, meaning AOD-9604, unlike CJC-1295 or tesamorelin, does not push the systemic hormone axis.
The flagship efficacy result is METAOD005: a Phase IIb 12-week randomized, double-blind, placebo-controlled trial of 300 obese subjects. The 1 mg/day group lost 2.8 kg on average. Placebo lost 1.0 kg. Statistically significant but absolutely small, and a 24-week follow-up trial saw the diet-and-exercise effect wash out the drug effect entirely. Metabolic Pharmaceuticals quietly pivoted away from obesity toward osteoarthritis and joint repair. The lipolytic mechanism is real in obese rodents. In healthy, lean, well-trained adults on a standard endurance diet, the effect on fat oxidation during exercise has not been characterized in a single randomized trial. AOD-9604 is not FDA-approved as a drug, was reclassified out of the 503A bulks pathway, and is prohibited by WADA under S2.
MOTS-c, CJC-1295, and the Mitochondrial Stack
MOTS-c gets endurance physiologists excited and anti-doping agencies nervous. Discovered in 2015 by Changhan David Lee and Pinchas Cohen at the USC Leonard Davis School of Gerontology, MOTS-c is a 16-amino-acid peptide encoded in the 12S rRNA region of the mitochondrial genome. It is one of a small family of mitochondrial-derived peptides that suggest mitochondria are not just power plants but active metabolic regulators. Circulating MOTS-c in humans rises about 1.6-fold during exercise and stays elevated about 1.5-fold post-exercise for roughly four hours, functioning as an exercise-induced mitokine that activates AMPK, the master metabolic switch also driven by metformin and caloric restriction. Marathon runners show higher resting MOTS-c levels than sedentary controls.
The 2021 Nature Communications paper everyone cites is mouse work: MOTS-c treatment doubled treadmill running capacity in old mice when started at 23.5 months, the late-life human equivalent. There are zero published human clinical trials of exogenous MOTS-c for athletic performance. WADA classifies it as prohibited under S0, and no therapeutic use exemption is available.
CJC-1295 sits in a different category. It is a growth-hormone-releasing-hormone analogue, often stacked with the GH secretagogue ipamorelin. Subcutaneous CJC-1295 dose-dependently raises plasma growth hormone by 2 to 10 times baseline for six days and elevates IGF-1 by 1.5 to 3 times baseline for up to 11 days. That is the entire reason people take it and the entire reason WADA bans it. Unlike sermorelin, the drug-affinity-complex modification keeps CJC-1295 pharmacologically active for days, producing sustained, supra-physiological GH elevation the body's somatostatin brake cannot fully control. We've covered the dosing economics in our piece on Hollywood's quiet CJC-1295 and ipamorelin protocols. The Topol cancer concern applies here too: chronic IGF-1 elevation has a theoretical signal for accelerating proliferation of clinically silent tumors, exactly the demographic risk profile of a 47-year-old runner already worrying about recovery.
Collagen, PeptiStrong, and What Actually Stays Legal
Two peptide categories survive the WADA filter, and they are also the two with the most human data. That is not a coincidence. Peptides that survive long enough to become regulated foods or supplements tend to do so because someone ran the trials.
Collagen peptides are the only peptide class with deep, extensive human RCT data. Daniel König's group at the University of Vienna has been the engine of this work. A 2024 systematic review and meta-analysis in Sports Medicine pooled 19 RCTs and reported that prolonged daily collagen peptide supplementation alongside training produces statistically significant improvements in fat-free mass, maximal strength, and tendon morphological adaptations. Most trials used 15 grams per day; emerging 2024 work suggests 30 grams may further increase collagen synthesis in resistance-trained subjects. A 2023 RCT by Centner, Jerger, and König had 55 male participants take 15 grams daily during 12 weeks of concurrent training. After 150 drop jumps, the supplemented group showed significantly improved post-jump maximal voluntary contraction, rate of force development, and countermovement jump height versus placebo. A separate trial reported improved one-hour running time-trial performance with the same dose. Tendon dry weight is 65 to 80 percent collagen; USADA explicitly states that collagen peptides are not prohibited.
PeptiStrong, the AI-discovered fava-bean-derived peptide, is what endurance influencers are starting to push as a legitimate alternative to underground compounds. Manufacturer-sponsored clinical studies report power output improvements up to 144% and performance increases up to 54% in trained individuals. Read those numbers with the usual industry-funded caveats, but they sit within the range academic BCAA trials have produced. PeptiStrong is sold as a food ingredient, not a drug, and is not on the WADA list. The companion PeptiSleep (rice bran) has shown a 17% deep-sleep increase and reductions in cortisol in smart-ring-instrumented trials. For a marathoner in a heavy training block, sleep quality is often a more useful intervention than yet another anti-inflammatory.
GLP-1 Drugs and Endurance: The Strange Exception
The counterintuitive line: GLP-1 receptor agonists like semaglutide and tirzepatide are currently permitted under WADA regulations. They are peptides. They are FDA-approved drugs (Wegovy, Ozempic, Mounjaro, Zepbound). They have the largest randomized human dataset of any peptide class. Roughly 12% of Americans are now taking them, with effects characterized across tens of thousands of patient-years of placebo-controlled data. They fall outside WADA's prohibited mechanisms because they do not increase GH, stimulate erythropoiesis, raise testosterone, or anabolic-affect muscle.
That gap has consequences. Some endurance athletes use GLP-1s to drop weight before goal races, and the muscle-mass loss in aggressive non-diabetic GLP-1 weight loss is real, well-characterized, and probably career-ending for a serious marathoner. Topol flags side effects beyond the gastrointestinal headlines: obstruction, excessive muscle loss, and emerging eye-disease associations. A six-month low-dose semaglutide course may produce a faster qualifier than three more months of training for a 39-year-old with 15 pounds to lose. That is supervised pharmacotherapy in a population the drug was not designed for, not a peptide hack.
The WADA and FDA Reality Check
The list of endurance-relevant peptides a tested athlete can use without ending their career is almost empty. S0 (Non-Approved Substances) covers BPC-157 explicitly, plus anything sold as "research use only" (Selank, Semax, SS-31, retatrutide, SLU-PP-332). S2 (Peptide Hormones, Growth Factors) covers TB-500, IGF-1, recombinant GH, EPO, CJC-1295, ipamorelin, GHRP-1 through GHRP-6, and tesamorelin. MOTS-c is prohibited under S4 Section 4.4 (Metabolic Modulators). The 2026 update expanded M.3 Gene and Cell Doping to cover nuclei, mitochondria, and ribosomes, and added non-diagnostic carbon monoxide use as a new prohibited method.
Strict liability catches recreational athletes off-guard. Athletes are responsible for any prohibited substance detected regardless of intent or origin. A contaminated supplement or mislabeled vial produces the same default four-year ban. No TUE is granted for experimental peptides used to recover from training. The FDA layer has sharpened in parallel. BPC-157's Category 2 reclassification is part of a broader pattern: GHRP-2, ipamorelin, and others moved to the same restricted category over two years. Professor Adam Taylor at Lancaster University warns that vials in this market can carry bacterial endotoxins capable of triggering septic shock.
Eric Topol's Critique and the Evidence Gap
Eric Topol, founder of the Scripps Research Translational Institute, has been blunt. In his 2025 Ground Truths essay "The Peptide Craze", he calls the trend "unfounded" and the evidence base "wanting." On the influencer stacking culture: "These influencers are often advocating taking a stack of peptides each month, so it could be two, three, four different peptides. This is really what I consider dangerous."
The structural argument is straightforward. BPC-157, TB-500, MOTS-c, and CJC-1295 share a common biology: they push cell growth, angiogenesis, or hormone-axis stimulation. Each carries a theoretical cancer risk because each can, in principle, supply a dormant tumor with the same growth signals it gives healthy tissue. None has a long-term human safety dataset adequate to characterize that risk. GLP-1 drugs by contrast went through animal models, phase I/II/III, and post-market surveillance across millions of patients. "There is no evidence from randomized trials in humans that any of these peptides provide the benefits that are advocated," Topol concludes, referring to the BPC-157 / TB-500 / MOTS-c / CJC-1295 cohort, not GLP-1s.
Brad Stanfield, a New Zealand GP and longevity researcher, makes the practical version of the same argument. The animal data is interesting; the absence of human trials makes self-administration "a gamble"; athletes wanting evidence-backed recovery should stick with creatine, sleep, and progressive overload. Lauren Reese, Kurt Wagner, and Henry Bone Ellis, writing for the American Orthopaedic Society for Sports Medicine, frame it from the clinician side: "the translational gap between rodent studies and meaningful clinical human studies is large," and recommending these substances is not within evidence-based sports medicine practice. The endurance peptide market has run ahead of the science. Collagen, GLP-1s, and AOD-9604 have real human data. Most of the rest do not.
Frequently Asked Questions
Are any peptides safe and legal for tested marathoners to use?
Yes. Collagen peptides are unrestricted and have the most robust human evidence base, including 19-RCT meta-analytic support for tendon adaptation, recovery from exercise-induced muscle damage, and one-hour time-trial performance at 15 grams per day. PeptiStrong (fava bean) and PeptiSleep (rice bran) are also food-grade ingredients, not synthetic peptide drugs, and are not on any WADA list. GLP-1 receptor agonists are technically permitted but carry serious muscle-mass-loss risk and were not designed for performance use.
If BPC-157 is banned, why do telehealth clinics still prescribe it?
The legal status changed in January 2025 when the FDA moved BPC-157 to Category 2, removing it from the 503A bulks pathway most compounding pharmacies had been using. Some clinics adjusted; others continued through gray-market or research-chemical channels. WADA has prohibited BPC-157 since 2022, but WADA enforcement only applies to athletes in tested sports. There is no general law prohibiting non-athletes from possessing it. The combination of regulatory gap, telehealth prescribing pressure, and weak enforcement of the FDA reclassification has produced the current confused picture.
Does collagen actually help tendons heal faster?
The Sports Medicine 2024 meta-analysis of 19 RCTs found that 15 grams of specific collagen peptides daily, taken alongside training, produces statistically significant improvements in tendon morphology and strength over weeks-to-months timelines. The mechanism is consistent with availability of glycine, proline, and hydroxyproline as building blocks for new collagen synthesis. The effect is real but modest. Collagen is not a substitute for progressive load management or rest from a structural injury.
How serious is the cancer risk from peptides like TB-500 or CJC-1295?
Theoretical for healthy users; no long-term human cohort has been tracked. The mechanism concern is biologically defensible: peptides driving angiogenesis or chronic IGF-1 elevation can, in principle, accelerate proliferation of clinically silent malignancies. For anyone with a cancer history, a family history of certain cancers, or a current screening abnormality, that theoretical concern becomes clinically meaningful. Most clinicians who prescribe these compounds screen out high-risk patients.
What about microdosing GLP-1 drugs for marathon weight loss?
Increasingly common in recreational endurance circles. GLP-1s are FDA-approved with extensive safety data, but they were not designed for lean athletes. The muscle-mass loss that accompanies the weight loss is real and meaningful at the marathon level. Talk to a physician who understands endurance physiology, not a longevity clinic with a monthly-subscription financial interest.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











