What copper peptides and retinol actually do in skin
If you want the blunt answer: retinol is the better-proven wrinkle treatment. Copper peptides are the more forgiving repair ingredient. That sounds like a dodge, but it is the most honest way to read the evidence.
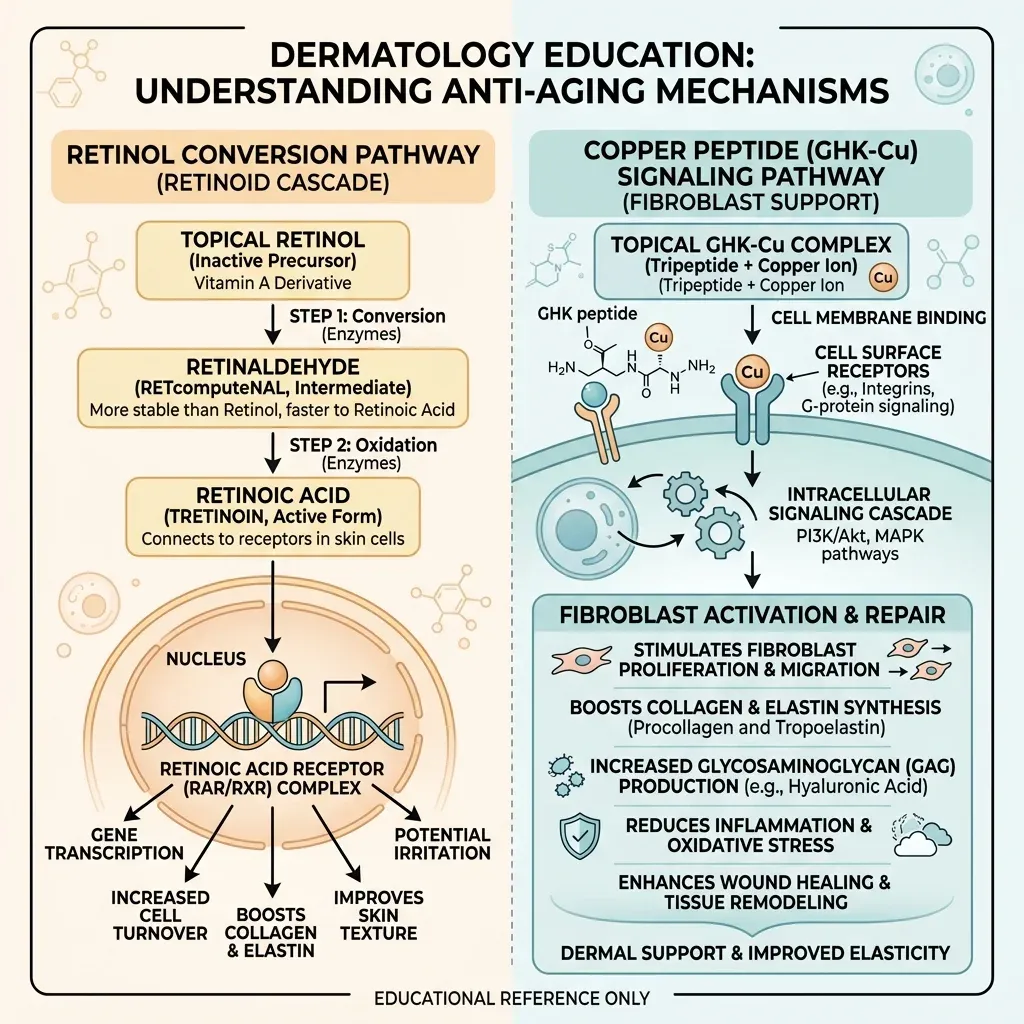
Retinol belongs to the retinoid family, which means it sits on the vitamin A family tree with retinaldehyde, tretinoin, adapalene, and tazarotene. The catch is conversion. After topical use, retinol has to pass through retinaldehyde before becoming retinoic acid, the active form that skin cells can use according to a focused clinical review in Advances in Therapy. Think of retinol as a prepaid card that still needs activation at the register. Tretinoin is already activated.
Once retinoic acid is available, it works more like a manager changing the shift schedule than like a scrub. Retinoids bind nuclear receptors in skin and change gene transcription programs tied to epidermal growth, differentiation, and dermal repair as summarized in a clinical efficacy and safety review of retinoids. That is why good retinoid results look gradual: smoother texture first, then fine-line changes, then better tone if the skin tolerates the process.
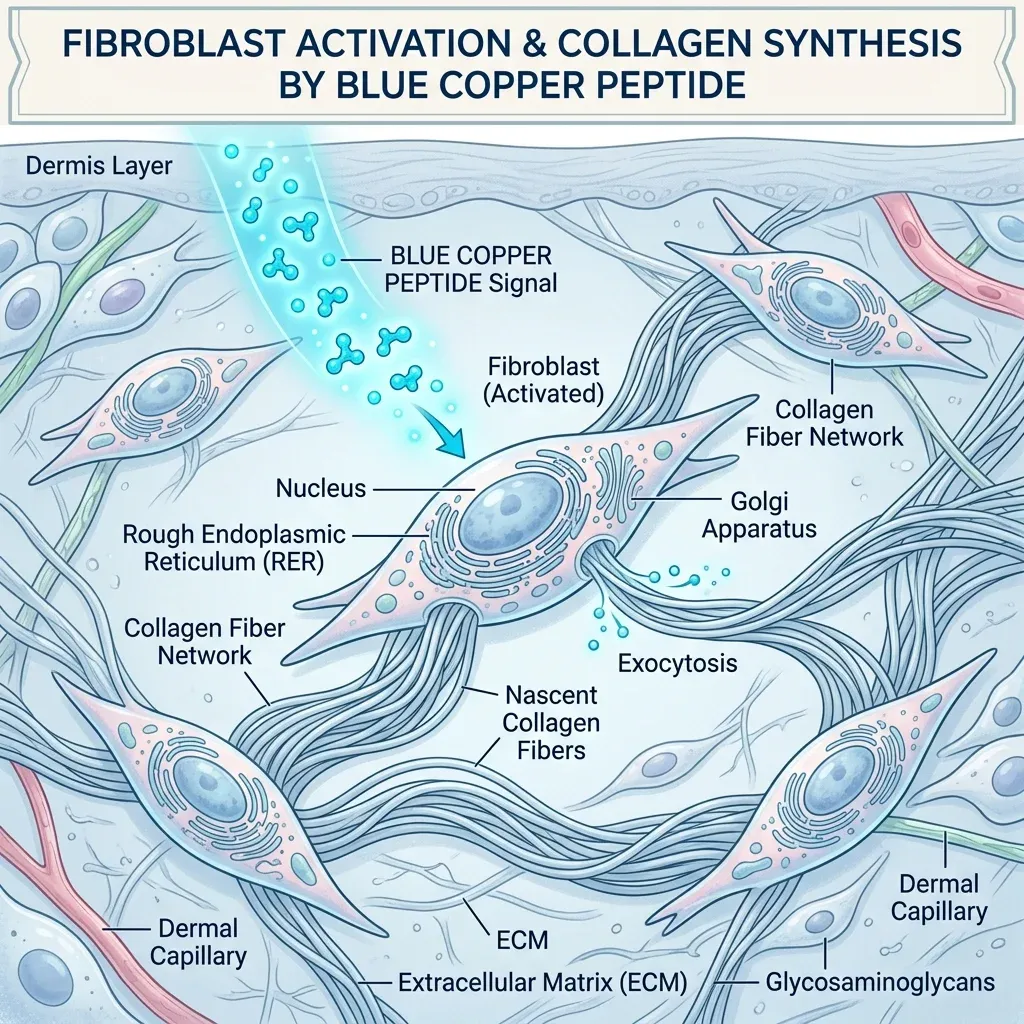
Copper peptides are playing a different game. GHK is a naturally occurring peptide that binds copper to form GHK-Cu, and the complex has been studied for tissue remodeling, wound repair, antioxidant effects, and anti-inflammatory signaling in a review on GHK as an anti-aging peptide. If retinol is the renovation crew stripping old wallpaper, copper peptides are closer to a site foreman telling fibroblasts which repair materials to bring.
The strongest biological case for GHK-Cu is not that it peels skin faster. It appears to support collagen, elastin, glycosaminoglycan synthesis, and dermal fibroblast function in a review of GHK-Cu's regenerative actions. That makes copper peptides more interesting for barrier-weary skin than for someone demanding a dramatic wrinkle reset by next month.

Where the wrinkle evidence is strongest
The wrinkle-proof contest is not close if we include prescription retinoids. A systematic review and meta-analysis by Huang and Lee identified 8 randomized tretinoin trials with 1,361 patients and follow-up lasting from 16 weeks to 2 years. In that analysis, topical tretinoin significantly improved fine wrinkles with a mean difference of 0.412 and coarse wrinkles with a mean difference of 0.245 compared with vehicle in photodamaged facial skin.
That does not mean every retinol cream on a store shelf deserves the same halo. A systematic review of over-the-counter vitamin A cosmetic products found 9 randomized, double-blind, vehicle-controlled retinol trials; 4 reported no statistically significant difference from vehicle. The authors judged the positive trials as weak evidence for mild fine-line improvement and warned that the flaws were serious enough to question whether those results should guide clinical decisions for cosmetic retinol products.
Still, retinol itself is not empty marketing. In a randomized, double-blind, vehicle-controlled left-right arm study, topical 0.4% retinol was applied up to 3 times weekly for 24 weeks in naturally aged skin. Fine-wrinkling scores changed by -1.64 with retinol versus -0.08 with vehicle, and the difference was statistically significant at P<.001 in the same PubMed-indexed study. Small biopsy subgroups also showed increased glycosaminoglycan expression and procollagen I immunostaining after retinol treatment.
A newer 12-week double-blind randomized trial gives a more modest real-world number: 0.5% retinol improved wrinkle severity by 4.11% in a head-to-head study comparing retinol with oleyl adapalenate. That is useful context. Retinol can work, but it is not magic. The better your formula, dose, consistency, and sunscreen habits, the more likely you are to see the slow payoff.
Why retinol still wins the proof contest
Retinol wins because it belongs to the better-tested family. In the retinoid literature, tretinoin is repeatedly described as the gold standard and the best-studied topical retinoid for antiaging treatment in a focused clinical evidence review. Tretinoin and tazarotene are also the retinoids in that review with approved indications for photoaged skin as adjunctive treatment rather than cosmetic-only positioning.
The important nuance is that "retinoid" and "retinol serum" are not interchangeable promises. Prescription tretinoin has the longest and strongest record. Cosmetic retinol sits lower on the potency ladder because the skin has to convert it into retinoic acid first according to the retinoid clinical review. That conversion is why retinol is usually easier to tolerate, and also why it may underperform a prescription retinoid.
The FDA-labeling story is sobering too. The OTC vitamin A review notes that Renova, a tretinoin 0.02% product, received FDA approval for mitigation of fine facial wrinkles in people using comprehensive skincare and sunlight avoidance, but the labeling says it does not eliminate wrinkles, repair sun-damaged skin, reverse photoaging, or restore younger skin according to the review's FDA-label discussion. Translation: even the proven ingredient is not a time machine.
The best practical takeaway is not "buy the strongest retinoid." It is "respect the biology." If your skin can handle retinoids, they remain the more evidence-backed route for fine wrinkles and photodamage. If your skin cannot handle them, the best clinical evidence in the world will not help you if you quit during the early irritation ramp.
This is also why the internet argument gets muddled. People compare a gentle copper peptide serum against the worst week of an overzealous retinol routine, then conclude the peptide is "better." That is not an evidence comparison; it is a tolerability comparison. The fairer comparison is a slow retinol ramp against a consistently used peptide product, with sunscreen held constant. In that match, retinol still has the stronger wrinkle data, while copper peptides make the routine easier to live with.
Where copper peptides may have the edge
Copper peptides have a weaker direct wrinkle-trial base than retinoids when compared with the retinoid clinical review literature, but they have a better temperament. That matters for real faces. Many people do not fail retinol because the science is poor; they fail it because their skin gets dry, red, tight, or flaky before the benefits arrive.
GHK-Cu's repair argument starts with age biology. Human serum GHK averages about 200 ng/mL at age 20 and declines to about 80 ng/mL by age 60 according to a review of GHK as an anti-aging peptide. That does not prove that replacing it topically reverses aging, but it explains why researchers keep looking at it: the molecule is tied to tissue remodeling signals that decline with age.
The skin data are intriguing. Pickart and Margolina's GHK-Cu review reports that, in fibroblast work combining GHK with LED irradiation, cell viability increased 12.5-fold, bFGF production rose 230%, and collagen synthesis rose 70% compared with LED irradiation alone in the reviewed experimental data. The same review reports that a 12-week thigh-skin study found GHK-Cu improved collagen production in 70% of treated women versus 50% with vitamin C cream and 40% with retinoic acid in the cited comparison.
There are also small topical studies. A 12-week facial cream study in 71 women with photoaging signs reported increased skin density and thickness, reduced laxity, improved clarity, and reduced fine lines and wrinkle depth in the GHK-Cu review. A 12-week eye-cream study in 41 women reported better performance than placebo and vitamin K cream for lines, wrinkles, skin density, and thickness around the eye area.
There is also a small but useful mechanistic bridge between the two ingredients. In a serum-free fibroblast model, McCormack, Nowak, and Koch tested copper tripeptide and tretinoin on normal and keloid-producing dermal fibroblasts in a 2001 Arch Facial Plastic Surgery study. Tretinoin-treated normal fibroblasts produced more basic fibroblast growth factor at 24 hours, while copper-tripeptide-treated keloid-producing fibroblasts secreted less transforming growth factor-beta1 at 24 hours in the same experiment. That does not prove cosmetic wrinkle reversal, but it shows why these actives are not duplicates. They push different repair signals.
That is promising, but not a knockout. Dermatologist Jennifer Gordon's practical warning is the right one: GHK-Cu can support repair and collagen production, but it should not replace retinoids for wrinkle reduction in her dermatologist review of the trend. Copper peptides are the friendlier training partner, not the heavyweight champion.
Can you use copper peptides and retinol together?
You can build a routine around both, but "both" should not mean "pile everything on the same night and hope your skin negotiates." The fetched evidence did not include a large direct clinical trial testing same-routine copper peptide plus retinol layering for wrinkle outcomes, while the retinoid trials and GHK-Cu studies were evaluated separately in retinoid reviews and in GHK-Cu reviews. So the cautious answer is based on mechanism, tolerability, and common retinoid side effects rather than a clean head-to-head stack trial with known retinoid irritation risks.
Retinoids commonly cause what the literature calls a retinoid reaction: pruritus, burning, erythema, and peeling, especially in the first weeks according to the retinoid safety review. DermNet lists retinoid dermatitis with erythema, peeling, dry skin, and irritant contact dermatitis among topical retinoid adverse effects in its topical retinoid guidance. It also advises sunscreen and moisturizer support because topical retinoids can worsen sun sensitivity and dryness during use.
A 180-day pilot retinol formulation study shows the rhythm of that adjustment period in people with moderate-to-severe photoaging. In the first 4 weeks, 81% of participants had at least one retinoid-associated effect, mostly mild erythema, peeling, and dryness in the pilot study's safety data. By day 180, 76.2% reported no adverse events after the step-up protocol. The annoying part is the lesson: irritation often gets better, but the ramp matters.
A sensible routine treats retinol night like leg day. Do the demanding work, then recover. Start with fewer retinol nights, buffer with moisturizer, and keep copper peptides for non-retinoid nights or morning use if the product directions allow. If your skin stings, flakes, or turns shiny-tight, the problem is not a lack of dedication. It is a routine asking too much from the barrier.
One more rule keeps the comparison honest: do not use copper peptides to excuse a chaotic active-heavy routine. If you are already using exfoliating acids, prescription acne medication, vitamin C, or a strong retinoid, the recovery side of the routine needs to be boring. Cleanser, moisturizer, sunscreen, and one repair serum is plenty. A copper peptide can be part of that quieter lane, but it should not become one more complicated step in a bathroom chemistry experiment.

The practical winner depends on your skin
Choose retinol if your priority is the best-supported wrinkle pathway and your skin can tolerate a slow ramp. Choose copper peptides if your skin is reactive, post-procedure, dryness-prone, or already irritated from acids and retinoids. Choose both only if you are patient enough to separate them and read your skin's feedback.
Retinol is less irritating than tretinoin, but it is also less potent and must be converted into retinoic acid before doing its full work according to the retinoid review. That middle-ground status is exactly why it is popular. It gives many people a tolerable entry point into the retinoid world.
Copper peptides deserve a different expectation. Use them when the goal is better-feeling, more resilient skin over time, not a prescription-strength resurfacing effect. If your face gets tight and shiny after every retinol attempt, a copper peptide serum may help you stay in the anti-aging game without constantly provoking redness. If your skin already tolerates retinol beautifully, copper peptides are optional support rather than the main event.
There are clear caution zones. DermNet notes that some topical retinoids are contraindicated in pregnancy and that tazarotene carries teratogenic concern in its safety guidance. The broader retinoid safety review advises caution in pregnancy because systemic retinoids are known teratogens, even though topical absorption is limited in long-term topical-use discussions. Anyone pregnant, trying to conceive, breastfeeding, or dealing with significant skin disease should get individualized medical guidance rather than crowdsourcing a routine.
The anti-wrinkle winner is retinoids for proof, copper peptides for repair support, and neither if you skip sunscreen.
So who wins? Retinol wins the anti-wrinkle battle on evidence, especially when we judge it as part of the retinoid family. Copper peptides win the comfort-and-repair lane. For many adults, the smartest routine is not a duel. It is retinol doing the remodeling work at a tolerable pace, copper peptides supporting recovery, and sunscreen preventing the daily collagen damage that no serum can fully outrun.

Frequently Asked Questions
Is copper peptide better than retinol for wrinkles?
No, not if the question is direct wrinkle evidence. Retinoids have the stronger clinical trial base for fine wrinkles and photodamage in randomized tretinoin trials. Copper peptides are better viewed as supportive repair ingredients, especially for people who struggle with irritation.
Can I use copper peptides on the same night as retinol?
The safest practical approach is to separate them at first. The fetched research did not include a large direct trial proving same-routine copper peptide plus retinol layering improves wrinkles, while retinoid irritation is well documented in dermatology guidance. Alternate nights or use copper peptides in a lower-irritation part of the routine.
How long does retinol take to improve wrinkles?
Published retinol and retinoid studies commonly evaluate outcomes over weeks to months. One 0.4% retinol study ran for 24 weeks and found significant fine-wrinkle improvement versus vehicle after that treatment period. Expect gradual change, not overnight tightening.
Are copper peptides gentler than retinol?
Usually, yes in practical skincare terms, because copper peptides are not forcing the same retinoid adjustment reaction. Retinoids can cause burning, erythema, peeling, and dryness in the first weeks according to retinoid safety reviews. Copper peptides can still irritate some people, so patch testing is still sensible.

Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.










