What GLP-1 Actually Does in Your Body
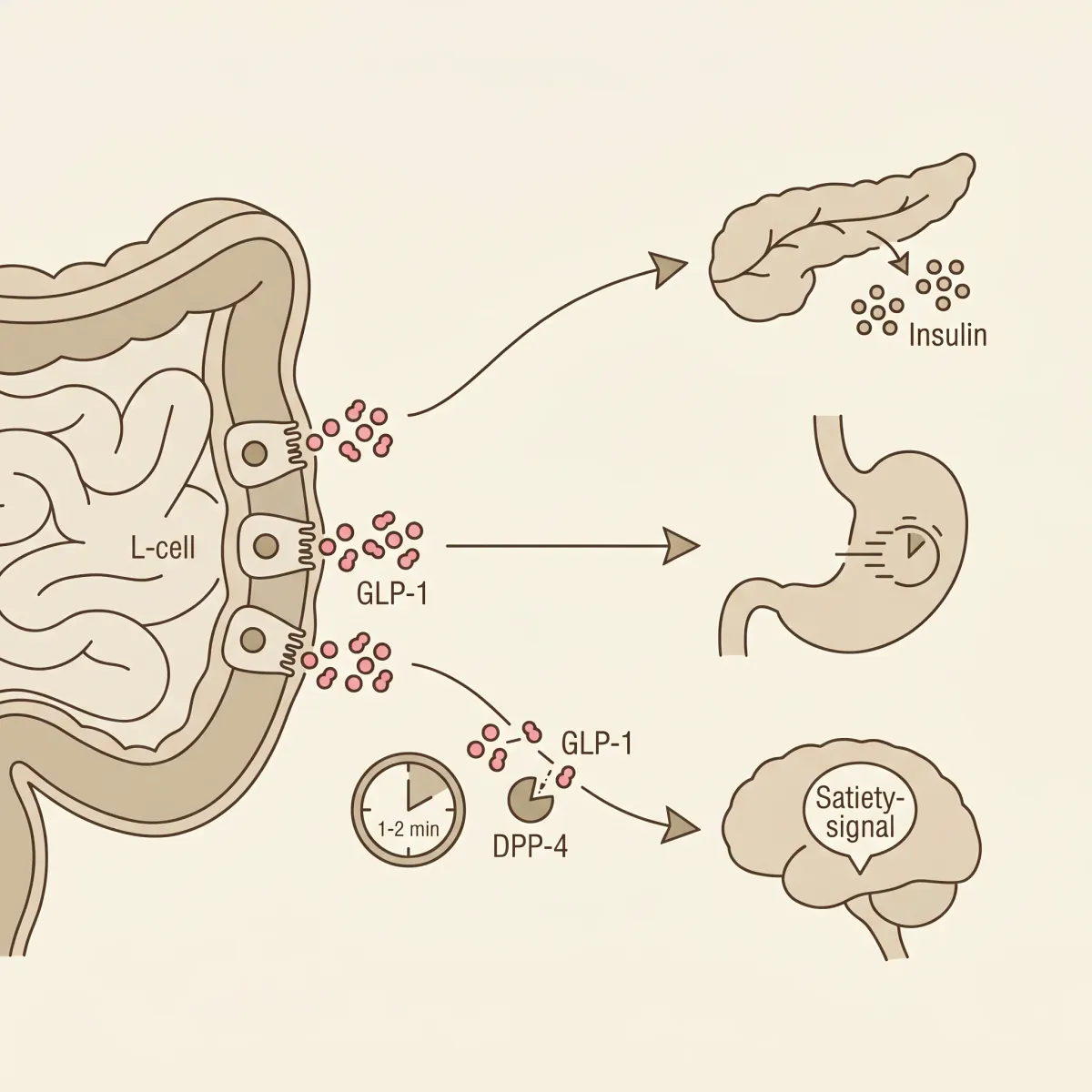
Picture the moment after you finish a meal. Within minutes, specialized cells lining your small and large intestine (called L-cells) sense the food and release a hormone called glucagon-like peptide 1, or GLP-1. This is the same hormone that drugs like Ozempic and Wegovy mimic. The catch is that your body has been doing this for free, every time you eat, your entire life.
GLP-1 works four jobs at once. It tells your pancreas to release insulin so blood sugar doesn't spike. It suppresses glucagon, the hormone that pushes glucose up. It slows down how fast food leaves your stomach, which keeps you feeling full longer. And it signals the appetite-regulation centers in your brain that it's time to stop eating, according to a review of GLP-1 secretion mechanisms published in PMC and clinical guidance from the Cleveland Clinic.
The GLP-1 your body produces from a meal has a half-life of only 1 to 2 minutes. An enzyme called dipeptidyl peptidase-4 (DPP-4) sits in your bloodstream and snips GLP-1 apart almost as fast as it is released, as the same PMC review documents. The whole reason semaglutide exists is that pharmaceutical chemists redesigned the GLP-1 molecule so DPP-4 cannot recognize and destroy it, turning a 2-minute hormone into a once-weekly injection, according to a perspective article in the Journal of Nutrition.
That difference matters for what food can and cannot do. Diet-driven GLP-1 release happens in pulses tied to each meal, fades within minutes, and over the course of a day produces an average weight reduction of roughly 5 to 7%. GLP-1 receptor agonist medications, by comparison, average closer to 20% weight reduction, also per the Journal of Nutrition perspective. Food cannot match the magnitude. What it can do is shift the baseline of every meal in a direction that compounds over months and years, without the nausea, the cost, or the rebound weight gain when you stop.
How Food Triggers Your Gut to Release GLP-1
Your L-cells do not respond to "food." They respond to specific molecules, and they have at least three different sensors for picking those molecules up.
The first sensor responds to amino acids, especially branched-chain ones like leucine and isoleucine. The second responds to fatty acids, particularly the monounsaturated kind found in olive oil and avocados, by activating a receptor called GPR120 (sometimes labeled FFAR4) on the L-cell surface. The third sensor reacts to short-chain fatty acids, or SCFAs (acetate, propionate, and butyrate), which are not in food directly. Gut bacteria produce them by fermenting dietary fiber that survives the small intestine intact, and those SCFAs bind to receptors called FFAR2 and FFAR3 on L-cells in the colon, according to a 2025 study from the University of Aberdeen published in Frontiers in Microbiology.
Think of it this way. Your small intestine is a chemical greeter that handshakes with proteins and fats as soon as a meal arrives. Your colon is a slow-cooker staffed by trillions of bacteria. Whatever fiber you ate eight hours ago is still being broken down in there, releasing little bursts of SCFAs that keep nudging GLP-1 release long after the meal itself is gone. Both stages matter; skipping fiber means you lose the long tail entirely.
This is where most modern diets quietly fail. The recommended daily intake of fiber for adults sits at 25 to 38 grams. The actual average for American adults is 16.3 grams, with only about 5% of the population hitting the adequate target, according to a 2024 perspective in the Journal of Nutrition. The slow-cooker is mostly empty.
The order in which you eat the food also turns out to matter. Eating protein, fat, or vegetables before carbohydrates produces a measurably higher GLP-1 response and lower post-meal blood sugar than eating carbs first, according to clinical guidance from Ohio State Health. Two people can eat exactly the same meal and finish with different glucose curves depending on which fork they pick up first. That's not a rounding error.
The practical takeaway: stack all three triggers at every meal (protein, healthy fat, and fermentable fiber), and bring the carbs in last. You aren't eating differently. You're eating in a different order with a different ratio.

The 5 Foods With the Strongest Evidence for Boosting GLP-1
The internet has lots of "10 foods that work like Ozempic" listicles. Most of them list whatever sounds healthy. The five below have actual peer-reviewed clinical or mechanistic evidence behind them, meaning either a controlled human trial measured GLP-1 directly, or a well-mapped molecular pathway shows how the food triggers L-cell secretion.
1. Avocado
A 2019 randomized clinical trial by Zhu and colleagues tested whether eating a whole avocado at breakfast changed satiety hormones. Compared to a calorie-matched control meal, the avocado meal raised GLP-1, raised peptide YY (another satiety hormone), and lowered insulin, as documented in Healthline's review of GLP-1-stimulating foods citing the original PMC-indexed study. Avocados pair their generous fiber content with a heavy dose of monounsaturated fat, meaning a single fruit simultaneously hits the GPR120 fat sensor in the small intestine and feeds the SCFA-producing bacteria in the colon.
2. Eggs
A 2016 review by Bodnaruc and colleagues in Nutrition and Metabolism assembled the human trials on protein-driven GLP-1 release, as cited in a News-Medical analysis. The standout finding: replacing a bagel breakfast with three eggs lowered post-meal blood glucose, reduced subjective hunger, and decreased calorie intake over the following 24 hours. Eggs also happen to be dense in leucine and isoleucine, the two amino acids most directly tied to L-cell GLP-1 secretion in mechanistic studies.
3. Extra Virgin Olive Oil
A 2021 research review summarized in Healthline's foods-that-increase-GLP-1 piece concluded that olive oil, and particularly the extra-virgin grade, increases GLP-1 secretion through its monounsaturated fat content. The newer angle is on the polyphenols. Compounds like oleocanthal and hydroxytyrosol, found in unrefined olive oil, appear to inhibit DPP-4, the enzyme that destroys GLP-1, according to reporting in NutritionInsight. Most foods just boost GLP-1 release. Polyphenol-rich olive oil may also extend how long the GLP-1 you have already released stays active. That's a meaningful difference if you're stacking these effects across an entire day.
4. Oats and Barley
The soluble fiber concentrated in oats and barley is called beta-glucan. In an 18-week study at the University of Aberdeen, mice on a high-fat diet supplemented with oat beta-glucan lost body fat compared to controls. Researchers traced the effect to elevated colonic butyrate, one of the SCFAs that triggers GLP-1 via FFAR2 and FFAR3 receptors, per the Frontiers in Microbiology study. Beta-glucan is also why oatmeal has a measurable cholesterol-lowering effect; the two mechanisms (cholesterol binding in the small intestine, SCFA production in the large intestine) run in parallel.
5. Greek Yogurt and Whey-Rich Dairy
A 2009 cell-line study by Chen and Reimer tested how isolated dairy components affected GLP-1 release in human intestinal cells. The results were unusually clean: 2% leucine produced a 4.7-fold increase in GLP-1 secretion, isoleucine 2.6-fold, casein 2.5-fold, and skim milk 1.6-fold, as reported in a PMC review of multiple GLP-1 secretion factors. Greek yogurt is also unusually protein-dense, since the straining process concentrates casein and leucine into a much smaller volume than ordinary yogurt. A 2021 review confirmed that whey, casein, soy, and gluten proteins all stimulate GLP-1 release in humans, also cited by Healthline.
Quick Reference
| Food | Primary GLP-1 Trigger | Best Evidence |
|---|---|---|
| Avocado | Fiber + monounsaturated fat (GPR120 + SCFAs) | 2019 RCT — Zhu et al. |
| Eggs | Leucine, isoleucine, complete protein | 2016 review — Bodnaruc et al. |
| Extra virgin olive oil | Oleic acid (GPR120) + DPP-4-inhibiting polyphenols | 2021 research review |
| Oats & barley | Beta-glucan → SCFA butyrate (FFAR2/FFAR3) | 2025 Frontiers study (mouse model) |
| Greek yogurt | Leucine + casein | Chen & Reimer 2009 (cell line) |

Food-Based GLP-1 vs. Ozempic and Wegovy: What the Research Shows
This is the comparison nobody wants to give you straight. Dr. Mary J. Scourboutakos, a family physician who writes for The Conversation, ran the actual numbers. A Mediterranean-style diet (the most GLP-1-stimulating eating pattern in the published literature) produces a peak GLP-1 level of approximately 59 picograms per milliliter. The lowest dose of Ozempic produces a GLP-1 level of 65 nanograms per milliliter. One nanogram equals 1,000 picograms. Medications raise GLP-1 levels more than 1,000 times higher than diet, according to her analysis published via MedicalXpress.
That's not a typo, and it's not the whole story either.
Pharmaceutical GLP-1 agonists raise hormone activity to what clinicians call "supraphysiological" levels, far above anything the body produces in any natural state, as noted by Spa Black, a Texas medical weight-loss clinic. That's exactly why they work for severe obesity. It's also why roughly half of patients on GLP-1 receptor agonists discontinue treatment within one year, with discontinuation rates running 65% in non-diabetic patients and 47% in patients with type 2 diabetes, according to the Journal of Nutrition perspective. The supraphysiological levels that produce 20% weight loss also produce nausea, vomiting, gastric paresis, and rebound hunger when the drug is stopped, as GLP-1 levels collapse.
| Mediterranean Diet | Ozempic (lowest dose) | |
|---|---|---|
| Peak GLP-1 level | ~59 pg/mL | ~65 ng/mL (65,000 pg/mL) |
| Average weight loss | 5–7% | ~15–20% |
| Discontinuation at 1 year | n/a | ~50% |
| Cardiac event risk reduction | ~30% | Variable by drug |
The Mediterranean diet's cardiovascular track record actually compares favorably with newer drug data. Long-running cohort studies have shown the diet lowers risk of cardiac events by roughly 30%, an effect that Scourboutakos argues outperforms the cardiovascular benefit of most GLP-1 medications studied to date.
So which is "better"? It depends on the goal. If you have type 2 diabetes, severe obesity, or metabolic syndrome that hasn't responded to lifestyle changes, the supraphysiological route exists for a reason. If you're aiming for steady, durable metabolic health on a timeline measured in years rather than weeks, food-driven GLP-1 release is what your physiology is built to do. The two aren't actually in competition. They're tools that fit different problems.
Drugs raise GLP-1 by 1,000-fold and produce dramatic short-term effects. Food raises GLP-1 by roughly 1.5- to 5-fold per meal and produces durable long-term effects. Choose based on which problem you're actually solving.

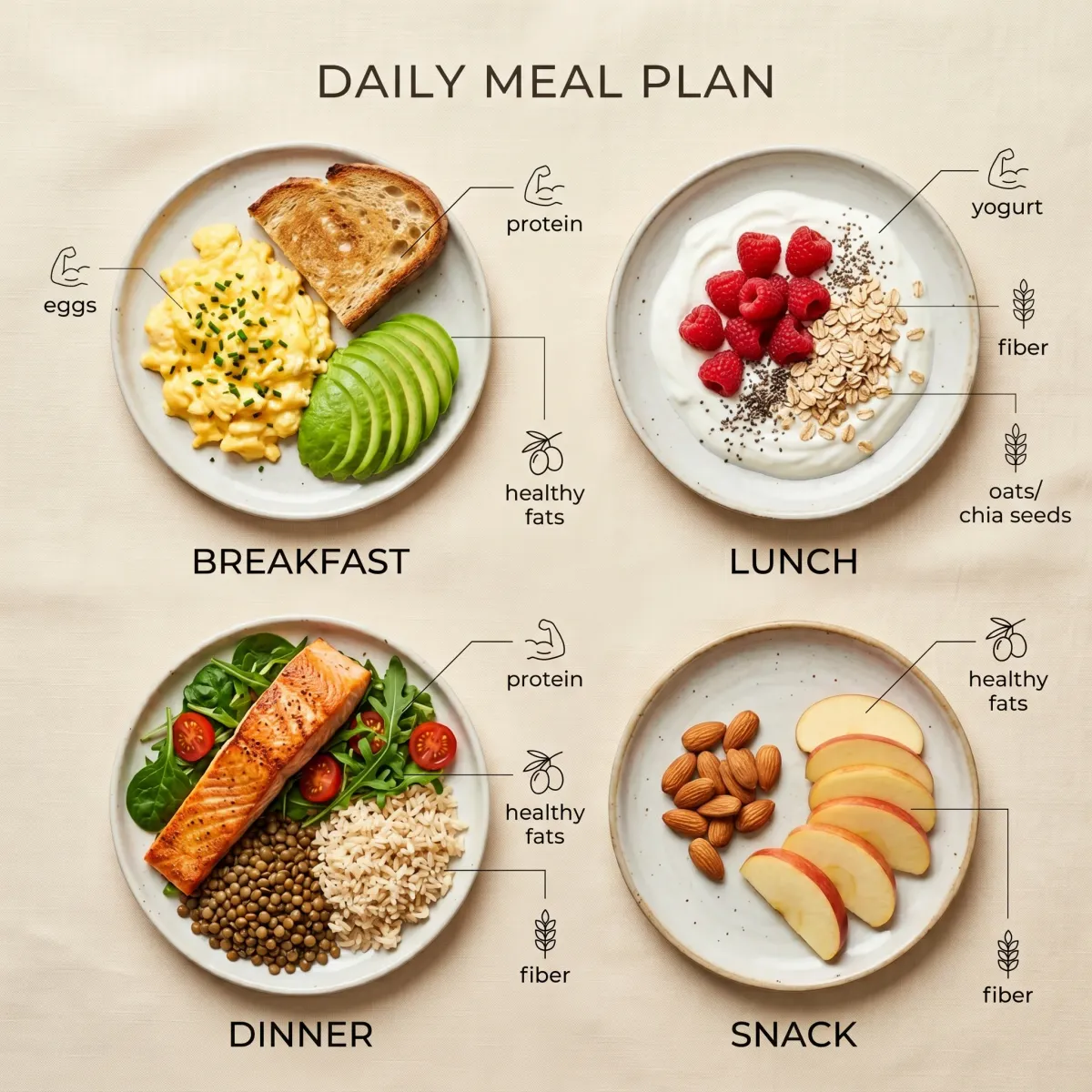
How to Build a GLP-1-Boosting Day of Eating
The five foods aren't the assignment. The assignment is to engineer every meal so it triggers all three GLP-1 sensors at once (amino acids, healthy fat, fermentable fiber), with carbohydrates entering last.
A workable day looks like this:
| Meal | Build | What it triggers |
|---|---|---|
| Breakfast | 3 scrambled eggs in 1 tbsp olive oil + 1/2 avocado + a slice of sprouted-grain toast eaten last | Leucine + GPR120 + fiber → carbs after |
| Lunch | Greek yogurt parfait: 1 cup plain non-fat Greek yogurt + 1/2 cup raspberries + 2 tbsp rolled oats + cinnamon | Casein/leucine + beta-glucan + polyphenols |
| Dinner | Salmon or chicken thighs roasted with olive oil, leafy greens, lentils. Vegetables and protein eaten before any rice or potato | Protein + MUFAs + fermentable fiber + meal sequencing |
| Snack | Small handful of almonds + apple slices | MUFAs + pectin (fermentable fiber) |
The simple target is 30 grams of fiber per day, the level recommended by the UK Scientific Advisory Committee on Nutrition for general metabolic health, according to clinical guidance summarized at Geisinger Health and a 2026 MDPI review on nutritional approaches to enhancing GLP-1. Hitting it requires real protein at every meal too, since amino acids and fiber together are more potent than either alone. This isn't about adding "superfoods." It's about redesigning portion sizes.
A few small extras have decent mechanistic support. Curcumin from turmeric, catechins from green tea, and certain other polyphenols appear to both stimulate GLP-1 secretion and modestly inhibit DPP-4, extending the active window of the GLP-1 you do release, according to a synthesis of bioactive compounds research. The effects are modest, not transformative. The center of the strategy stays the macronutrient stack at every meal.
One honest caveat worth sitting with. Most clinical trials that directly measure food-driven GLP-1 are short, often single-meal or single-day studies. The longer studies of weeks or months of eating this way mostly track downstream outcomes (weight, fasting glucose, A1c) rather than GLP-1 itself. The mechanism is solid; the long-term real-world data on how a high-fiber, high-protein, MUFA-rich pattern translates into sustained GLP-1 elevation is still being filled in. You're nudging a system, not flipping a switch. Go in with reasonable expectations.
Frequently Asked Questions
Can natural GLP-1 boosters replace Ozempic for serious weight loss?
For most people seeking moderate weight loss and metabolic improvement, food-driven GLP-1 release is sufficient and far more sustainable. For severe obesity (BMI > 35), type 2 diabetes that hasn't responded to lifestyle change, or insulin resistance with cardiovascular risk, the 1,000-fold higher GLP-1 levels produced by medications are doing something food cannot replicate. The decision should be made with a doctor who knows your full picture, not based on whether the drug is currently trendy.
How long until I notice effects from boosting GLP-1 with food?
Acute effects (more fullness during a meal, less drive to snack afterward) can show up within a single meal, particularly when you eat protein and vegetables before carbs. Measurable changes in weight, blood sugar, and waist circumference typically take a couple of months of consistent eating, and the gut microbiome shifts that drive SCFA production take a similar window to stabilize. There's no overnight version of this, which is also part of the appeal: it doesn't fail dramatically either.
Do probiotics or fermented foods help boost GLP-1?
The evidence here is mixed. Some sources point to specific strains like Lactobacillus reuteri as GLP-1-supportive, while clinical reviewers flag insufficient human evidence to recommend any specific probiotic strain for GLP-1 enhancement. What does have evidence: feeding the bacteria you already have via fermentable fiber. Yogurt, kefir, kimchi, and sauerkraut are healthy foods, but the GLP-1 effect from any of them mostly comes from the protein and fiber they contain, not the live cultures themselves.
Is intermittent fasting compatible with these GLP-1-boosting foods?
Yes. Intermittent fasting compresses your eating window but doesn't change what triggers GLP-1 when you do eat. The macronutrient stack (protein, fat, fermentable fiber, carbs last) works the same whether you eat it at noon or 8 a.m. One nuance worth knowing: research suggests GLP-1 release may be more pronounced earlier in the day than late evening, so front-loading the day's largest meal is plausibly more effective than a late dinner, though this finding is preliminary.
Related Articles
- The 7 Most Effective Weight Loss Peptides Doctors Are Quietly Recommending in 2026
- Tirzepatide vs. Semaglutide: Which GLP-1 Peptide Actually Melts More Fat?
- The GLP-1 Side Effect List Your Doctor Probably Won't Mention
- GLP-1 Microdosing: The Quiet Trend Replacing Full-Dose Ozempic in 2026
- Why Tirzepatide Users Lose 22% of Their Body Weight — and What Happens When They Stop
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.