
The $1,300 vs. $200 Price Gap: Where the Money Actually Goes
A month of brand-name Ozempic costs $499 at Novo Nordisk's direct patient price without insurance. At list price before any discounts, it runs higher. A month of compounded semaglutide from a 503A pharmacy typically costs $100-250, depending on the dose and the pharmacy.
That is a price difference of 50-80%. The semaglutide molecule in both products is the same amino acid sequence. So where does the money go?
The answer splits into three buckets: what Novo Nordisk spent before it could sell a single pen, what it spends now to keep selling pens, and what compounding pharmacies do not spend at all.
Novo Nordisk invested billions in clinical trials, regulatory submissions, manufacturing scale-up, and the delivery device engineering that produced the Ozempic pen. Those costs are amortized across each unit sold. A compounding pharmacy buys semaglutide API (active pharmaceutical ingredient) from a manufacturer and compounds it into a vial. No clinical trials. No NDA filing. No pen engineering. No television advertising budget.
The compounding pharmacy's costs are real but fundamentally different: pharmaceutical-grade API, compounding labor, sterility testing, facility overhead, and regulatory compliance. These costs are small relative to a multinational pharma company's R&D and marketing machine.

Why Brand-Name GLP-1s Cost What They Do: R&D, Patents, and Marketing
Novo Nordisk and Eli Lilly did not stumble onto semaglutide and tirzepatide. The GLP-1 receptor agonist class took decades of research to develop, starting with the discovery of GLP-1's role in glucose regulation in the 1980s and progressing through multiple generations of molecules (exenatide, liraglutide, dulaglutide) before arriving at the current blockbusters.
The clinical trial programs alone represent billions in spending. SURMOUNT (tirzepatide) and STEP (semaglutide) enrolled thousands of patients across multiple countries. The FDA approval process for each indication (type 2 diabetes, then obesity, then cardiovascular risk reduction) required separate trial programs.
Then there are patents. As Harvard health policy researchers explain, "they're patent-protected, so generic drug manufacturers can't produce these compounds for another few years. The companies that make these products are effectively monopolists." A generic version of Ozempic will not be available until at least 2033 due to patent protection in the United States.
Internationally, the timeline differs. Semaglutide's patent has already expired or will expire in 2026 in several countries including India, Canada, China, Brazil, and Turkey, which together represent 40% of the world's population and an estimated 33% of adults living with obesity.
Marketing adds another layer. Novo Nordisk and Eli Lilly run direct-to-consumer advertising campaigns that cost hundreds of millions annually. The Ozempic jingle is arguably the most recognized pharmaceutical ad of the decade. Every commercial, sponsored search result, and influencer partnership is built into the unit price.
How Compounding Pharmacies Hit 80% Less: The API Economics
Compounding pharmacies do not develop drugs. They buy the active ingredient and formulate it into a patient-specific medication. The economics of that process are dramatically simpler than a pharmaceutical company's.
The semaglutide API itself costs a fraction of the finished product price. Research by Dr. Andrew Hill at the University of Liverpool found that a new oral semaglutide formulation could be manufactured at a cost of approximately $16 per month. That figure covers the raw material and basic manufacturing, not the clinical trials, regulatory approval, or marketing that brand manufacturers need to recoup.
A 503A compounding pharmacy adds its own costs on top of the API price:
| Cost Component | Brand-Name (Novo Nordisk) | 503A Compounding Pharmacy |
|---|---|---|
| API (raw ingredient) | Manufactured in-house at proprietary scale | Purchased from FDA-registered API supplier |
| Clinical trials | Billions over 10+ years | $0 (not required) |
| FDA drug approval | NDA/BLA filing + review fees | $0 (compounds under 503A exemption) |
| Delivery device | Engineered autoinjector pen | Standard vial + syringe |
| Marketing | Hundreds of millions/year DTC advertising | Minimal (prescriber referral-based) |
| Quality testing | Full cGMP with in-house QC labs | Batch COA, sterility testing, state board compliance |
| Profit margin | ~80-85% gross margin (estimated) | ~30-50% (typical pharmacy margin) |
The 80% savings is not a mystery. It is the math of removing R&D amortization, clinical trials, regulatory approval, device engineering, and mass-market advertising from the price while keeping only the API and compounding costs.
What You Give Up (and What You Don't) at the Lower Price Point
Compounded semaglutide is not the same product as Ozempic. The molecule is the same. The rest is not.
What you keep: The same active peptide sequence. The same mechanism of action (GLP-1 receptor agonism). The same dose-response relationship. A prescription from a licensed provider. Medication compounded under state pharmacy board oversight (if from a legitimate 503A pharmacy).
What you give up: FDA review of the specific finished product. The standardized delivery device (pen injector). Long-term stability data on the specific formulation. The clinical trial data was generated using the brand product, not the compounded version. Post-market safety surveillance at scale. And since the semaglutide shortage ended, the legal basis for compounding it.
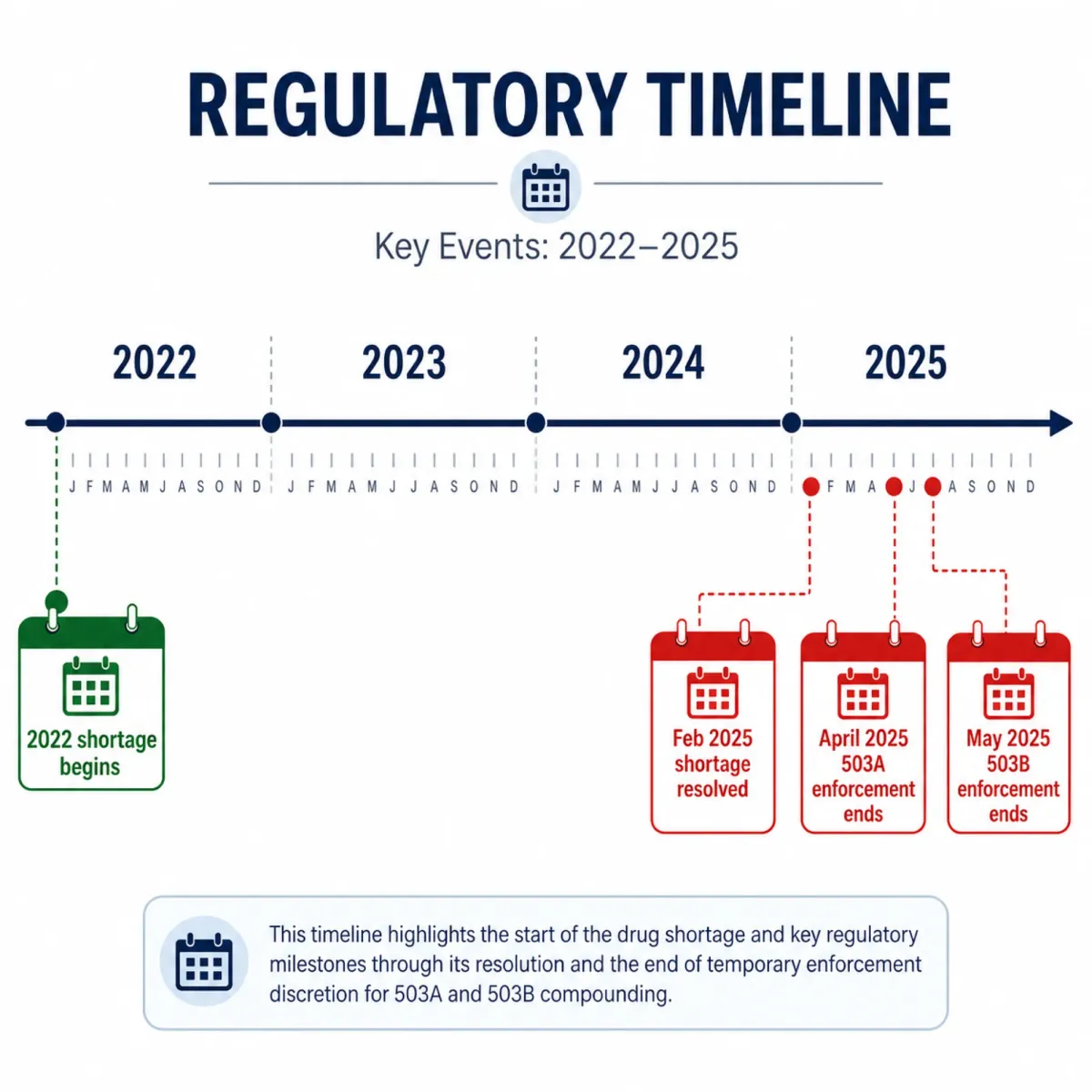
That last point is critical and widely misunderstood. Compounded versions of commercially available drugs are only legal when the drug is on the FDA drug shortage list or when the compounded version contains a "clinically meaningful difference" documented by the prescriber. The semaglutide shortage was resolved in February 2025. The legal window for compounding it has closed.
The Drug Shortage Loophole That Made Compounding Legal (and Its Expiration)
The compounded GLP-1 market was built on a legal mechanism that was never designed to be permanent.
Under Section 503A, compounding pharmacies cannot regularly make "essentially copies" of commercially available drugs. When semaglutide went on the FDA Drug Shortage List in 2022, the restriction lifted. Compounders could legally prepare semaglutide formulations because the brand product was not reliably available.
The FDA resolved the semaglutide shortage on February 21, 2025. Enforcement discretion for 503A pharmacies ended April 22, 2025. For 503B outsourcing facilities, it ended May 22, 2025. The tirzepatide shortage was resolved even earlier, on December 19, 2024.
The FDA has explicitly stated that tirzepatide and semaglutide do not currently appear on the 503B bulks list or on the drug shortage list. Any pharmacy still compounding semaglutide as an "essentially copy" of Ozempic or Wegovy is operating outside its legal authority.
Some compounders have argued that their formulations contain meaningful differences (different salts, combined with other ingredients like B12 or L-carnitine). The FDA has pushed back, clarifying that a compounded drug combining semaglutide with another API like vitamin B12 may still be considered an essentially copy if strengths and route of administration are comparable. The FDA's grace threshold: four or fewer prescriptions of that compounded product per calendar month.
Insurance, Coupons, and the Real Out-of-Pocket Math
The sticker price of GLP-1s is misleading because very few patients pay it. The out-of-pocket cost depends entirely on your coverage type.
| Coverage Type | Typical Monthly Out-of-Pocket | Key Conditions |
|---|---|---|
| Commercial insurance + manufacturer savings card | As low as $25/month | Must have qualifying insurance plan; savings card from Novo Nordisk |
| Commercial insurance, no savings card | $50-200/month | Varies by plan; prior authorization often required |
| No insurance (manufacturer direct price) | $499/month (Ozempic) | Novo Nordisk direct price program |
| No insurance, new Wegovy pill | $150/month | Announced pricing for oral formulation |
| Medicare Part D | $50/month (new deal) | Trump admin negotiated deals with manufacturers |
| Medicaid | Low or $0 | Only a few states cover anti-obesity medications; administrative hurdles |
| Compounded semaglutide (while it was legal) | $100-250/month | Required prescription; shortage list status expired |
Medicare Part D does not cover drugs that treat obesity, though the CMS Medicare GLP-1 Bridge program is testing what expanded coverage would look like. The $50 monthly copay deal applies to GLP-1s prescribed for diabetes (where Medicare coverage already exists), not for weight loss alone.
The hidden cost of brand-name GLP-1s goes beyond individual premiums. Health insurers are passing along GLP-1 costs in the form of higher rates across the board, according to Harvard health policy researchers. The drugs' popularity and price are already driving up insurance premiums for everyone, not just users.
Where GLP-1 Pricing Is Headed in 2026-2027
Three forces are converging on GLP-1 pricing, and all point downward.
Force 1: International patent expiration. Semaglutide's patent has expired or will expire in 2026 in countries representing 40% of the world's population. Generic manufacturers in India, China, and Brazil are already positioning to produce off-patent semaglutide. While these generics cannot be sold in the US (where patents run to 2033), their existence creates global pricing pressure and demonstrates that low-cost production is technically feasible.
Force 2: Oral formulations. Novo Nordisk's oral semaglutide (Rybelsus, and the newer Wegovy pill) eliminates the injection device cost entirely. The Wegovy pill is priced at $150/month for uninsured patients, a significant reduction from the injectable price. Dr. Andrew Hill's research at the University of Liverpool suggests the manufacturing cost for an oral formulation is approximately $16 per month, leaving substantial room for further price compression.
Force 3: Political and regulatory pressure. The Inflation Reduction Act's Medicare drug price negotiation provisions, the $50 copay deals, and the CMS GLP-1 Bridge program all reflect political will to reduce GLP-1 costs. As Harvard researchers note, "in about the next five years or so, these patents will start to expire, and we'll have generic manufacturers making their own GLP-1s."
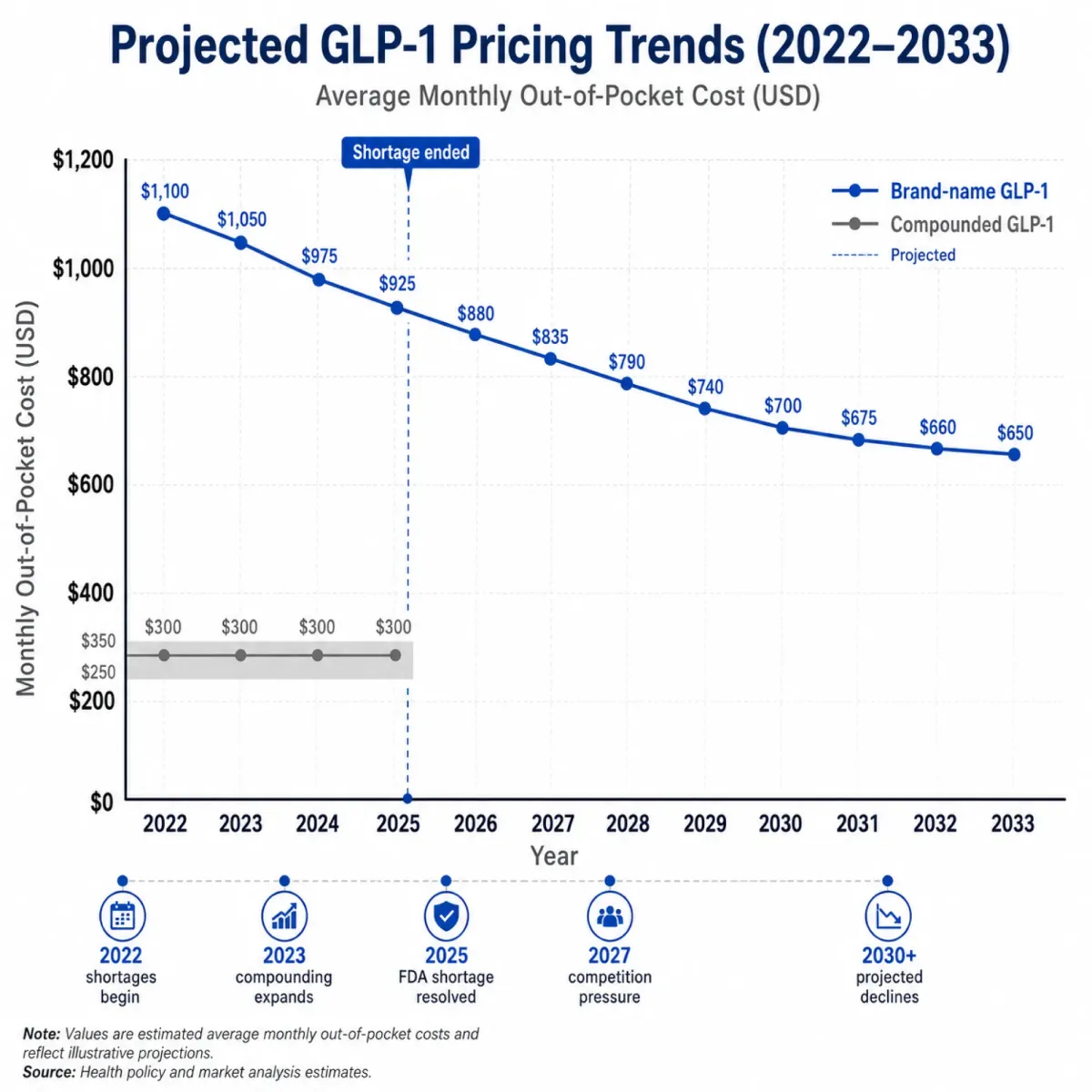
For the compounding market specifically, the trajectory is clear: the legal window for compounded GLP-1s has largely closed, and the brand-name price is declining toward a point where the compounding value proposition shrinks. The $1,300-vs-$200 gap that made compounding attractive in 2023 is becoming a $150-vs-$200 comparison that tilts toward the FDA-approved product.
Frequently Asked Questions
Is compounded semaglutide still legal to buy in 2026?
The legal basis for compounding semaglutide as an essentially copy of Ozempic or Wegovy expired when the FDA resolved the semaglutide shortage in February 2025. Some pharmacies continue to offer it through narrow compliance pathways (e.g., formulations with meaningful clinical differences), but the FDA has signaled aggressive enforcement. Compounded semaglutide from a 503A pharmacy without a valid legal basis carries regulatory risk for the pharmacy.
Why can't generic semaglutide exist in the US yet?
Novo Nordisk holds multiple patents on semaglutide that do not expire until at least 2033 in the United States. No generic manufacturer can produce semaglutide for the US market until those patents expire or are successfully challenged. Internationally, patents have already expired in countries like India and Canada, where generic production is beginning.
Does the $16/month production cost mean GLP-1s should cost $16?
The $16/month figure from Dr. Andrew Hill's research covers raw material and basic manufacturing costs for an oral formulation. It does not include clinical trials, FDA approval, quality assurance at scale, distribution, pharmacovigilance, or the profit needed to fund future R&D. Production cost is the floor, not the fair price. But the gap between $16 and $1,300 reveals how much of the current price reflects monopoly positioning rather than manufacturing reality.
Will Medicare cover GLP-1s for weight loss?
Medicare Part D currently does not cover drugs prescribed solely for obesity treatment. The CMS Medicare GLP-1 Bridge program is testing expanded coverage. The $50/month copay deal announced by the Trump administration applies to GLP-1s prescribed for diabetes, where Medicare coverage already exists. Legislative changes would be required for full obesity coverage under Part D.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











