Your face is losing more than fat
Something happens when you start losing weight on semaglutide or tirzepatide that nobody prepares you for. The scale drops, your clothes fit differently, and then you catch your reflection and barely recognize yourself. You look older.
That gaunt, hollowed-out appearance has a name. Dr. Paul Jarrod Frank, a cosmetic dermatologist in New York, coined the term "Ozempic face" after treating patient after patient whose faces seemed to age a decade in months. The term caught on, but the phenomenon is neither new nor limited to one medication.
"The term 'Ozempic face' refers to the changes in the face that can happen with rapid weight loss," says endocrinologist Dr. Vinni Makin of Cleveland Clinic. "It's characterized by gauntness, sunken cheeks, new wrinkles and loose skin on the face and neck." She points out that this isn't a side effect of the medication itself -- it's a consequence of how fast the weight comes off.
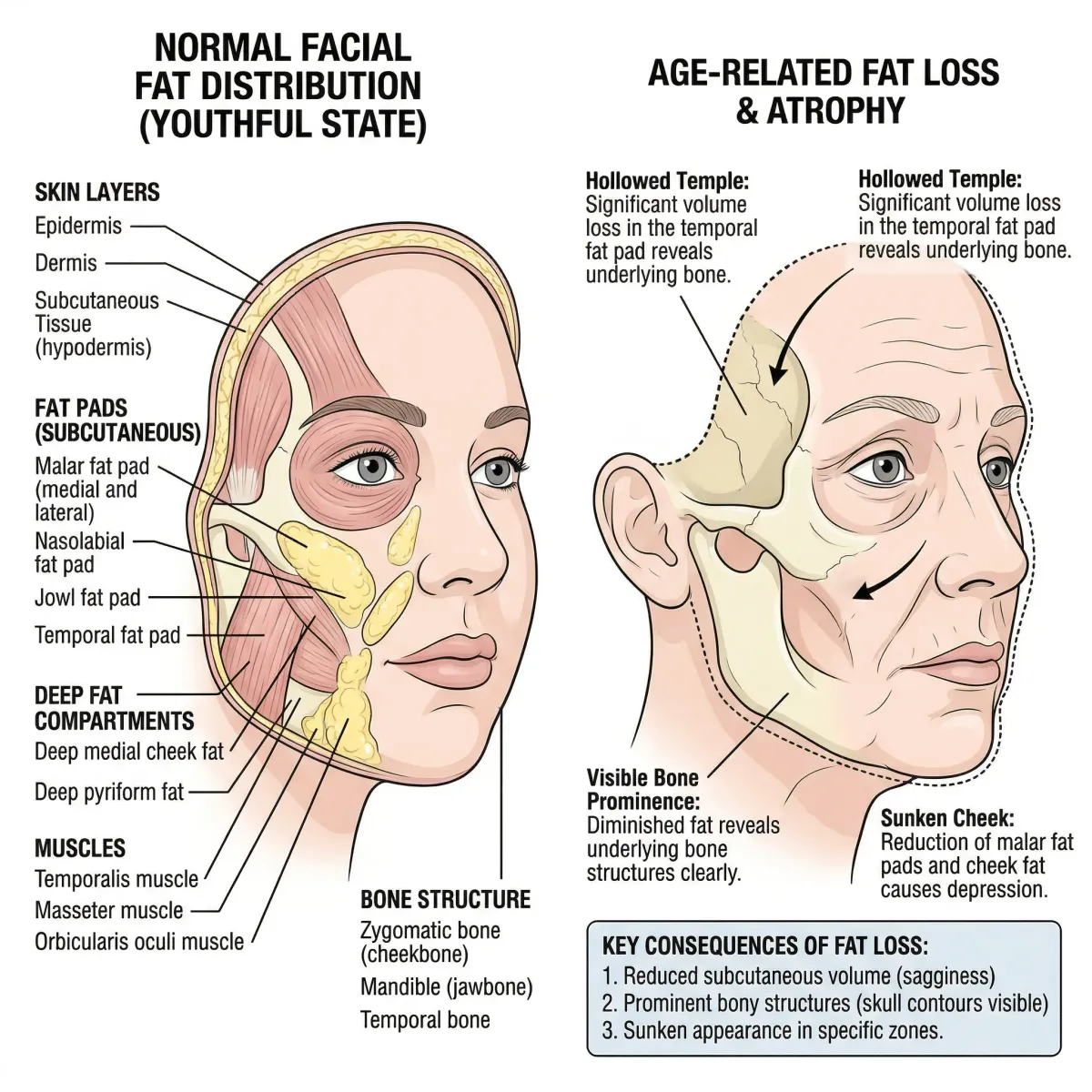
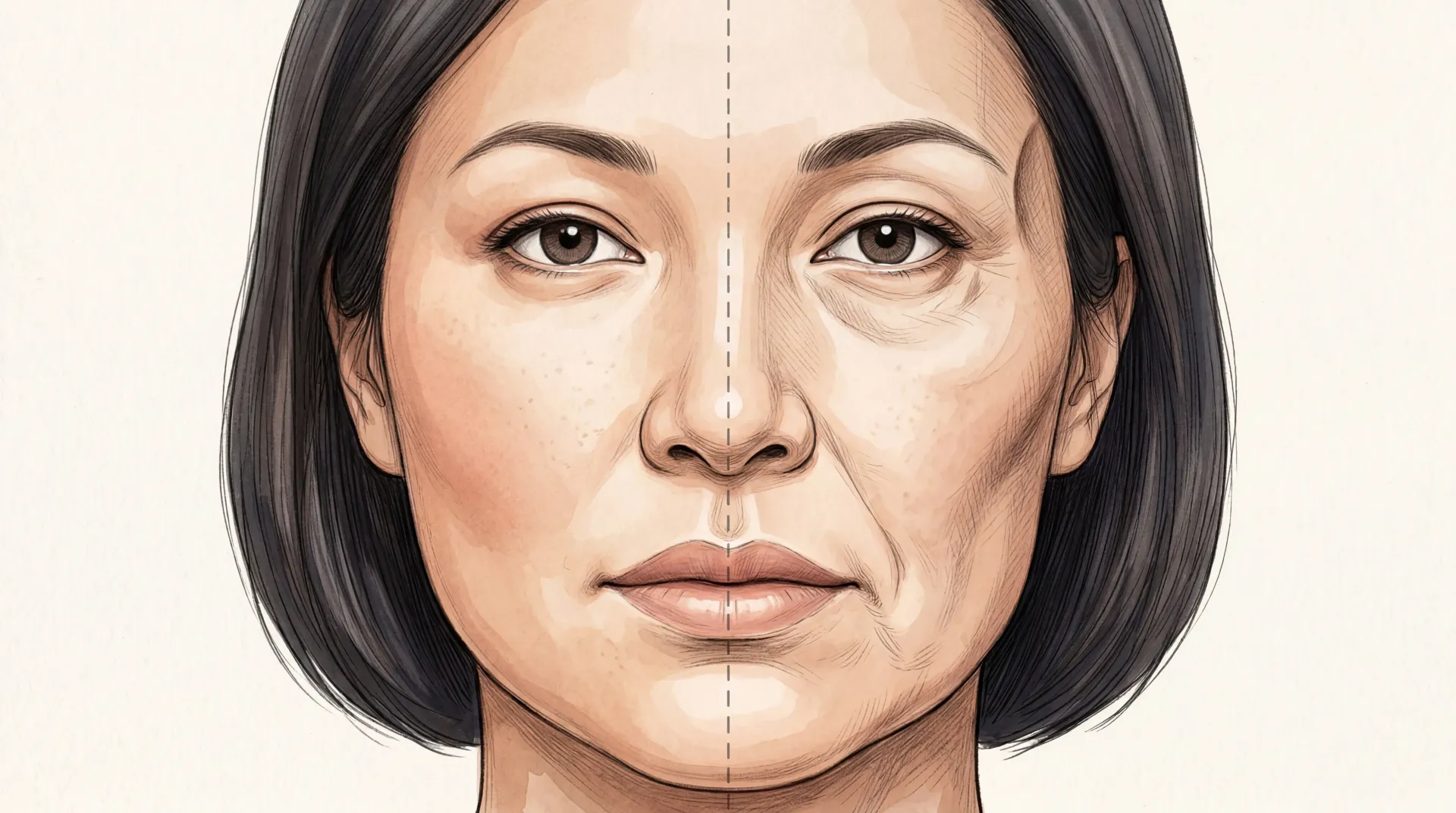
Your face works like a fitted sheet stretched over a mattress. The subcutaneous fat underneath acts as padding -- it gives your cheeks their fullness, your temples their smooth contour, your under-eye area its plumpness. When that padding disappears fast, the sheet doesn't shrink to fit. It sags, bunches, and wrinkles.
Rapid weight loss depletes the subcutaneous fat that supports facial structure. At the same time, elastin and collagen levels in the skin drop, removing the two proteins responsible for keeping skin tight. The result: sunken eyes, hollowed temples, prominent cheekbones where there used to be smooth contours, deeper nasolabial folds, and jowls along the jawline.
The scale of this is staggering. About 13% of American adults -- roughly 32 million people -- have used a GLP-1 receptor agonist at some point, according to a 2024 JAMA poll. About half are actively on a prescription. Millions of people are on a collision course with facial changes they may not have discussed with their prescriber.
Ozempic face is not a medical condition. It's a colloquial term for facial volume loss that accompanies any form of rapid, significant weight loss. Bariatric surgery patients, crash dieters, and people who've been seriously ill all experience similar changes. GLP-1 medications just produce dramatic, fast results that make facial changes impossible to ignore.
"You're just hearing about it more because so many more people are on this medication," says Dr. Andrea Bedrosian, a bariatric surgeon at Northwell Health. "Ultimately, it's just a sign of anybody who's losing a significant amount of weight in a short period of time."
The faster the weight drops, the worse the facial changes get. Patients on semaglutide in the STEP 1 trial lost 14.9% of their body weight over 68 weeks, compared to 2.4% on placebo. That kind of rapid loss gives skin no time to remodel, and the face -- where changes are most visible -- bears the brunt first.
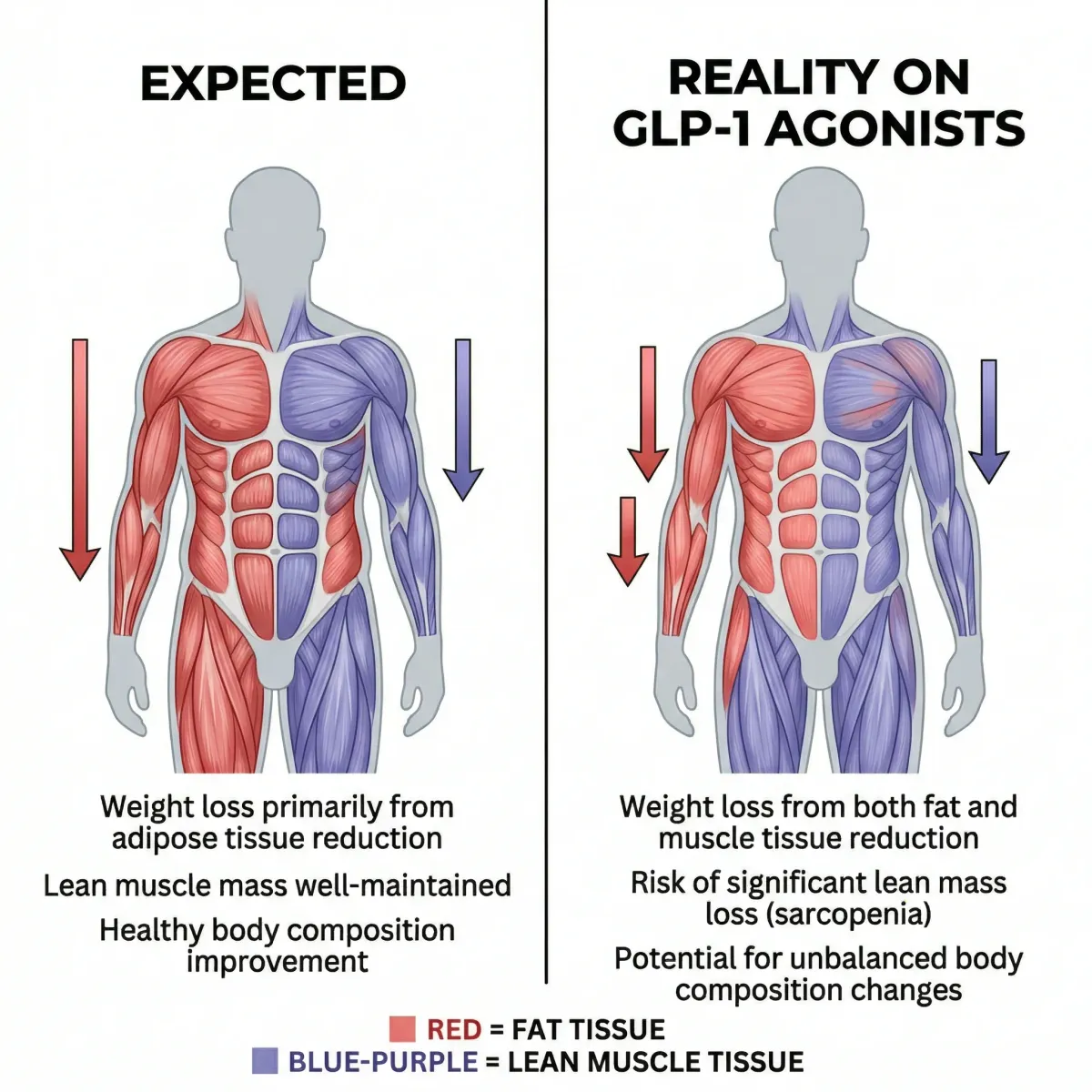
Up to 40% of the weight you're losing isn't fat
Weight loss on GLP-1 medications isn't just fat. A meaningful portion of what the scale registers as "weight lost" is lean tissue: muscle, organ mass, and water bound to glycogen stores.
The data is consistent and sobering. In the STEP 1 trial's DXA body composition subset, 95 participants on semaglutide lost 6.9 kg of lean soft tissue alongside 10.4 kg of fat mass. Roughly 40% of their total weight loss came from lean tissue. In the SURMOUNT-1 trial testing tirzepatide, 124 participants in the DXA subset fared somewhat better -- lean tissue accounted for about 26% of total weight lost (5.6 kg lean vs. 15.9 kg fat).
A systematic review analyzing six studies with 1,541 adults found lean mass reductions ranging from nearly 0% to 40% of total weight lost on semaglutide. A separate network meta-analysis placed the figure at about 25% across various GLP-1 and dual GLP-1/GIP receptor agonist drugs.
Why does this happen? Dr. Caroline Apovian, co-director of the Center for Weight Management and Wellness at Brigham and Women's Hospital, explains: "When you lose weight, you are decreasing caloric intake in terms of proteins, carbohydrates, and fats. The brain needs glucose. Fat by itself cannot be turned into glucose, and that is the major reason why muscle loss is inevitable when you decrease caloric intake."
Your body runs a grim calculation. The brain consumes about 20% of daily energy despite being 2% of body mass, and it runs almost exclusively on glucose. During a caloric deficit, your body breaks down muscle protein into amino acids, converts them to glucose through gluconeogenesis, and feeds that glucose to the brain. Fat can't do this job directly. Muscle gets sacrificed.
This isn't unique to GLP-1 medications. Dr. Armen Yerevanian, an endocrinologist at Massachusetts General Hospital, puts it this way: "We're not used to having successful weight loss outcomes at the scale we've seen with GLP-1 analogs, other than with bariatric surgery. Having concerns about lean body mass is reasonable, but GLP-1s are one tool of many for weight loss."
There is one encouraging data point. The SEMALEAN study followed 106 patients on semaglutide 2.4mg for 12 months. Lean mass declined initially -- about 3 kg by month 7 -- but then stabilized. Handgrip strength actually improved by 4.5 kg at month 12. The prevalence of sarcopenic obesity in the group dropped from 49% at baseline to 33%. The muscle that remained was functioning better, even if some had been lost.
The lean mass question is more nuanced than the 40% headline suggests. Some of that "lean" loss is water and glycogen associated with fat tissue, not contractile muscle fiber. But some of it is genuine muscle, and for your face -- which depends on that thin layer of subcutaneous fat for its structure -- the consequences show up in the mirror.
Not all GLP-1s hit your face equally hard
If lean mass loss drives facial volume changes, the obvious question is whether some GLP-1 medications are worse than others. The DXA data from clinical trials shows meaningful differences.
| Medication | Trial | Weight loss | Lean tissue as % of weight lost | Duration |
|---|---|---|---|---|
| Semaglutide 2.4mg | STEP 1 | 14.9% | ~40% | 68 weeks |
| Tirzepatide 5-15mg | SURMOUNT-1 | 15-21% | ~26% | 72 weeks |
| Liraglutide | Real-world cohorts | ~8% | ~22% | Varies |
Semaglutide at the full 2.4mg dose showed the highest proportion of lean tissue loss at ~40% in the STEP 1 DXA subset. Tirzepatide was better at ~26%, despite producing equal or greater total weight loss. As a narrative review in Frontiers in Endocrinology noted, real-world liraglutide cohorts report about 22% of total weight loss as lean mass.

Several factors beyond the specific drug determine how badly your face is affected:
- Speed of loss. The faster the weight drops, the less time skin has to remodel. Maximizing dose early to hit weight targets faster increases facial changes.
- Age. Older adults have lower subcutaneous fat reserves before starting treatment. They start with less facial padding, so any loss is more visible.
- Sex. Women and older adults with obesity may lose more muscle mass proportionally than younger men.
- Total weight lost. Losing 50-60 pounds produces more dramatic facial changes than losing 20-30 because more subcutaneous fat disappears.
- Face shape. People with longer face shapes may notice changes more because of how skin stretches over their bone structure.
If you're choosing between GLP-1 options and facial volume preservation matters to you, the DXA data suggests tirzepatide produces a more favorable body composition profile than semaglutide at equivalent weight loss. But the bigger levers are the lifestyle factors discussed next.
Protein and barbells: the two things that protect your face
The clinical trials that produced the alarming lean mass numbers had a critical design feature in common: no specific strength training protocol was included. Participants in STEP 1 and SURMOUNT-1 received counseling to achieve a 500 kcal/day deficit and 150 minutes/week of physical activity, but "physical activity" mostly meant walking. Nobody was squatting.
When researchers from Texas Tech University published a case series of patients who prioritized resistance training and protein intake while on semaglutide or tirzepatide, the results looked nothing like the clinical trial averages.
| Patient | Drug | Duration | Weight change | Fat change | Lean tissue change |
|---|---|---|---|---|---|
| Case 1: 42F | Tirzepatide | 115 weeks | -33.0% | -53.4% | -6.9% |
| Case 2: 42F | Semaglutide | 39 weeks | -26.8% | -61.6% | +2.5% |
| Case 3: 52M | Semaglutide then Tirzepatide | 139 weeks | -13.2% | -46.9% | +5.8% |
Look at the last column. Case 2 -- a 42-year-old woman on semaglutide -- lost 26.8% of her body weight but actually gained 1.2 kg of lean soft tissue. Case 3, a 52-year-old man, gained 3.8 kg of lean tissue while losing 14.1 kg of body weight. Even the worst result (Case 1) saw only 8.7% of weight loss come from lean tissue, compared to the 40% average in STEP 1.
What did these patients do differently? Two things, consistently.
Resistance training
All three patients performed resistance training 3-5 days per week. Not walking or cycling -- actual progressive strength work targeting all major muscle groups. The European Association for the Study of Obesity's Physical Activity Working Group has specifically noted that resistance training, not aerobic exercise alone, is what slows lean body mass loss during weight-loss diets.
The recommended minimum per combined WHO, ACSM, ADA, and EASO guidelines: 150 minutes of moderate aerobic activity per week plus resistance training 2-3 times weekly. But the case series patients who got the best results were doing more -- 3-5 sessions of strength work per week at moderate to high intensity.
Researchers at Mass General Brigham confirmed this. Combining a high protein diet and consistent exercise with GLP-1 treatment showed the greatest benefit in preserving bone and muscle mass, compared to diet alone or high protein alone. Patients who exercise from the start of treatment and keep it up throughout get the best body composition outcomes.

Protein: more than the standard recommendation
The standard RDA for protein is 0.8 grams per kilogram of body weight per day. For a 75 kg person, that's 60 grams -- roughly one chicken breast and two eggs. That's not enough when you're losing weight rapidly and trying to protect your muscle.
The case series patients consumed 0.7-1.7 g/kg/day relative to body mass, and 1.6-2.3 g/kg/day relative to fat-free mass. The patient who gained the most lean tissue (Case 2) aimed for 1.2-1.6 g/kg/day, consuming about 120 grams daily.
Multiple sources converge on the same recommendation: aim for 1 to 1.5 grams of protein per kilogram of body weight daily, with 20-30 grams at each meal. For a 180-pound (82 kg) person, that means 82-123 grams daily -- about double the RDA.
The GLP-1 appetite suppression that makes these drugs effective at causing weight loss is the same mechanism that makes eating enough protein difficult. When your appetite drops to nearly nothing, protein-rich foods -- meat, eggs, dairy -- that feel heavy and filling are often the first things patients skip. Protein shakes with at least 20 grams per serving become a practical tool here, not a supplement.
Slower is better
"Focus on slower weight loss -- about one to two pounds per week," Dr. Makin recommends. Maximizing dose to hit targets quickly works against facial preservation. Asking your prescriber about a slower titration schedule, or maintaining a lower maintenance dose once you've reached a target range, gives your skin more time to adjust and your body more time to preferentially burn fat over muscle.
From hyaluronic acid to fat grafting: what works
Prevention isn't always possible. For patients who've already developed significant facial volume loss, the question shifts to restoration. The options range from 15-minute office procedures to operating room surgeries. The right choice depends on timing, severity, and whether you're still actively losing weight.
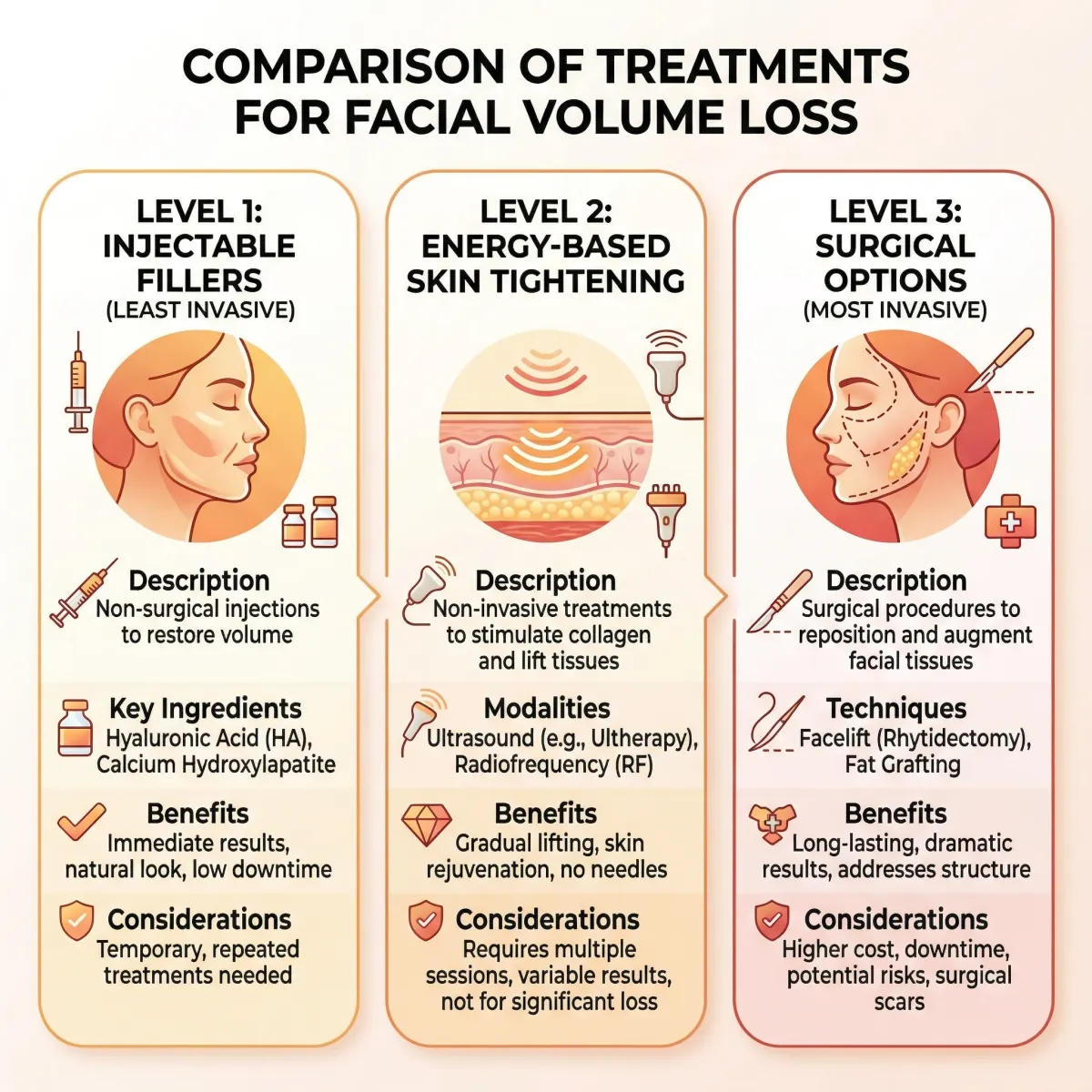
Injectable fillers: the first-line treatment
"Injectable fillers are the easiest way to re-volumize the face," says Dr. Mark Hamilton, a facial plastic surgeon and chairman of the public information committee for the American Academy of Facial Plastic and Reconstructive Surgery. "These can be done in the office with an immediate effect and little downtime."
Dr. Robyn Siperstein, a dermatologist who treats these patients daily, describes a specific protocol: start with the temples, which she identifies as "the biggest and most obvious sign of weight loss." From there, she moves downward -- cheeks and sub-malar hollows, then jawline and marionette area.
Technique matters as much as the product. Siperstein uses a higher G-prime (firmer) filler placed deep to replace the deep fat pads, then a softer, less cohesive hyaluronic acid filler more superficially to smooth contour changes. For patients who've lost significant subcutaneous fat, she switches from bolus injections to a cannula with a fanning technique because there's less fatty tissue to hide lumps and a higher risk of hitting blood vessels without the cushioning fat layer.
| Filler type | Mechanism | Best for | Timing | Duration |
|---|---|---|---|---|
| Hyaluronic acid (Juvederm, Restylane) | Immediate volume | Temples, cheeks, under-eyes, jawline | Anytime, even during active weight loss | 6-18 months |
| Sculptra (poly-L-lactic acid) | Stimulates new collagen production | Overall facial volume, skin texture | Only after weight loss is complete | 2+ years |
| Radiesse (calcium hydroxylapatite) | Immediate volume + collagen stimulation | Cheeks, jawline | After weight stabilization preferred | 12-18 months |
Timing is critical. Dr. Siperstein warns against using Sculptra during active weight loss: "If the body is losing weight, it is technically in what we call a starvation state, where there are not enough calories to keep up with the body's energy needs. When the body is in this state, it is keeping its energy for the vital organs... and will not have any excess energy to create more collagen." Hyaluronic acid fillers work through physical volume rather than biological stimulation, so they can be used at any point.
The best approach may be combination therapy -- Sculptra for longer-term collagen stimulation paired with HA fillers for targeted, immediate volume correction. But this should be staged over time. Dr. Siperstein recommends injecting slowly in stages rather than all at once because swelling from multiple syringes can distort the outcome.

Energy-based skin tightening
Noninvasive procedures like microneedling, platelet-rich plasma (PRP) injections, and radiofrequency (RF) skin tightening can reduce wrinkles and improve skin quality. These work by stimulating collagen remodeling in the dermis, tightening loose skin over time. They're most effective for mild to moderate laxity and work better as adjuncts to filler treatments than as standalone solutions for significant volume loss.
Surgical options
For severe cases, surgical interventions include cheek implants, fat grafting, and facelifts. Fat grafting -- where fat is harvested from one part of your body and injected into your face -- offers a more permanent solution than fillers, but requires enough donor fat and a surgical setting. Facelifts address skin laxity by repositioning or removing loose tissue from the face and neck.
Dr. Bedrosian recommends waiting before considering surgery. After significant weight loss, the skin needs time to adjust and may improve on its own. The degree of recovery depends on age, total weight lost, and how long someone carried the excess weight. Jumping to surgery too early means operating on a moving target.
When facial changes signal something worth addressing
Ozempic face doesn't bring negative health effects. It doesn't need treatment unless you want treatment. This is a cosmetic concern, not a medical emergency.
But there are situations where talking to your doctor makes sense:
- Rapid, dramatic changes in the first few months. This may indicate your dose is too high or your weight loss is faster than intended. A slower titration schedule could make a real difference.
- Signs of excessive muscle loss beyond the face -- difficulty with stairs, weakness, fatigue, loss of grip strength. The face is often just the most visible marker of a whole-body composition shift.
- Distress about your appearance. If facial changes are affecting your self-image or motivation to continue a medication that's improving your metabolic health, that's a legitimate conversation to have with your prescriber.
- Planning any procedure under general anesthesia. Ozempic should be discussed with your anesthesiologist before surgery because GLP-1 medications cause delayed gastric emptying, which affects anesthesia safety.
The changes won't reverse on their own. If you maintain your weight loss, the facial hollowing persists. If you regain weight, some fullness returns -- but that defeats the purpose of treatment. The goal is enough weight loss for metabolic benefit, managed at a pace that minimizes cosmetic effects, supported by protein and exercise that protect lean tissue.

Every expert interviewed across the research for this guide agrees on one thing: don't let fear of Ozempic face stop you from taking a medication that could transform your metabolic health. The obesity epidemic affects over 100 million American adults and contributes to $173 billion in annual healthcare costs. The benefits of GLP-1 medications for eligible patients -- reduced cardiovascular risk, improved blood sugar control, decreased all-cause mortality -- outweigh cosmetic side effects. Mitigate, don't avoid.
Frequently Asked Questions
Is Ozempic face permanent?
Facial volume loss from rapid weight loss does not reverse on its own. If you maintain your weight loss, the hollowed appearance persists. Cosmetic procedures like dermal fillers, fat grafting, or skin tightening treatments can restore volume. If you regain weight, some facial fullness may return, but this negates the health benefits of treatment and isn't recommended as a strategy.
Can you prevent Ozempic face entirely while still taking the medication?
Complete prevention isn't possible because you can't control where your body loses fat. Resistance training 3-5 days per week, consuming 1-1.5 grams of protein per kilogram of body weight daily, and working with your prescriber on a gradual weight loss pace of 1-2 pounds per week can significantly reduce severity. Patients in the Tinsley and Nadolsky case series who followed these strategies lost as little as 8.7% of their weight as lean tissue, compared to 40% in the STEP 1 trial where no strength training was prescribed.
How much do fillers for Ozempic face cost?
Costs vary based on the type and amount of filler needed, your geographic area, and the injector's experience. Patients with significant volume loss typically need multiple syringes across several sessions, and biostimulatory fillers like Sculptra require multiple treatments spaced weeks apart. These are cosmetic procedures not covered by insurance. Ask your dermatologist or facial plastic surgeon for an individualized treatment plan and cost estimate before starting.
Does tirzepatide (Mounjaro/Zepbound) cause less facial volume loss than semaglutide?
DXA body composition data from clinical trials suggests yes. In SURMOUNT-1, about 26% of weight lost on tirzepatide was lean tissue, compared to about 40% on semaglutide in STEP 1. Both drugs produce significant weight loss, but tirzepatide appears to have a more favorable fat-to-lean loss ratio. Individual results vary based on exercise habits, protein intake, and other factors.
Should I stop taking Ozempic if I notice facial changes?
Do not stop any prescribed medication without consulting your healthcare provider. Facial changes are a cosmetic concern, not a medical reason to discontinue treatment. Discuss strategies with your doctor: slower titration, dietary adjustments, or adding resistance training. If you stop GLP-1 treatment abruptly, research shows patients regain about two-thirds of lost weight within a year, which reverses the metabolic benefits.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











