A Yellow-Flowered Plant That Tricks Your Stress System
Somewhere in the rocky crevices above the Arctic Circle, a stubby perennial with yellow flowers clings to nutrient-poor soil and shrugs off temperatures that would kill most cultivated plants. Rhodiola rosea, also called golden root or arctic root, belongs to the Crassulaceae family and has been used medicinally in Russia, Scandinavia, and Tibet for centuries. The roots smell faintly of roses when cut, which is how Carl Linnaeus landed on the name.
What makes Rhodiola interesting to researchers is not its hardiness but what happens when you swallow an extract of its roots. Scientists have isolated more than 140 distinct compounds from R. rosea rhizomes, organized into six chemical groups: phenylpropanoids (the rosavins), phenylethanoids (salidroside and tyrosol), flavonoids, monoterpenes, triterpenes, and phenolic acids. The rosavins, a trio of compounds called rosavin, rosin, and rosarin, appear only in R. rosea and not in any other Rhodiola species, making them a reliable fingerprint for authenticating the real thing.
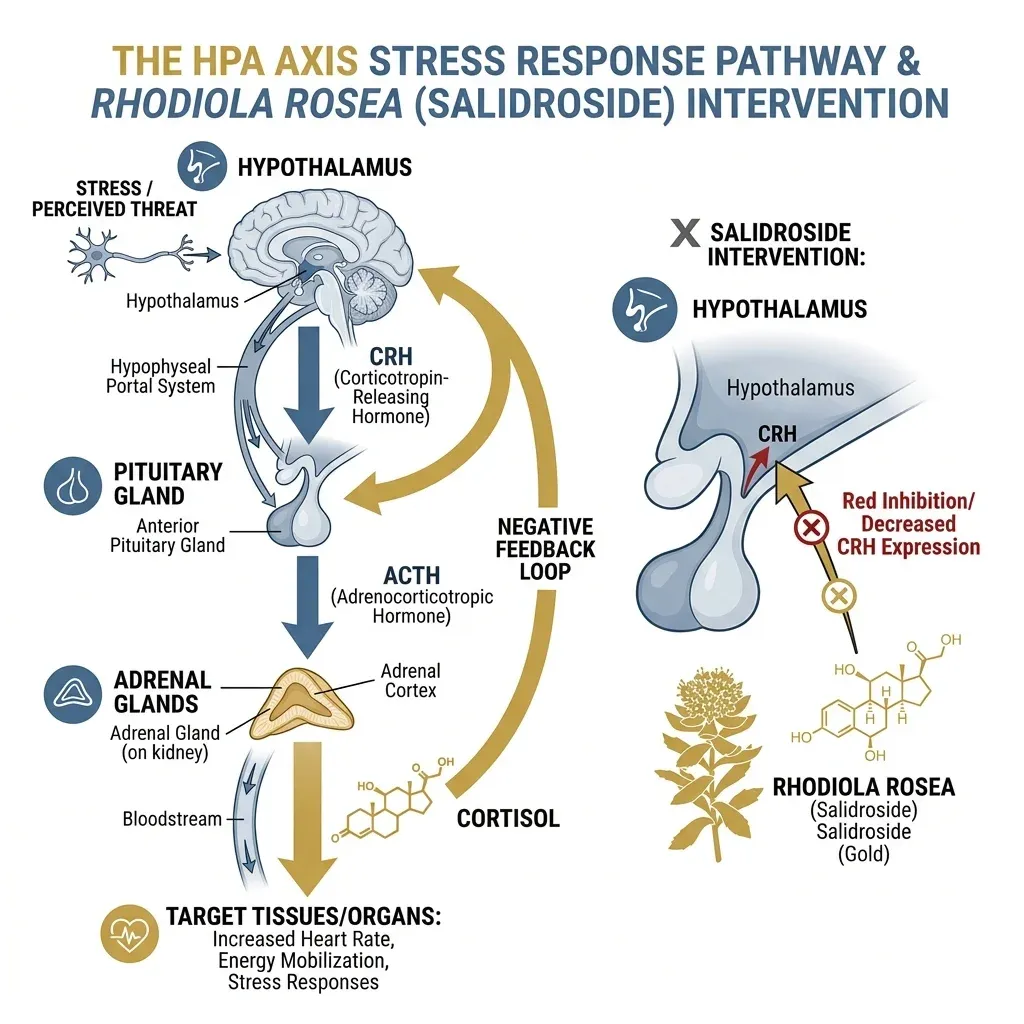
But knowing the ingredients tells you little about the mechanism. Think of your stress response like a thermostat: the hypothalamic-pituitary-adrenal (HPA) axis regulates how much cortisol and other stress hormones your body pumps out when something goes wrong. Rhodiola appears to recalibrate that thermostat. Salidroside, the compound most studied for its individual effects, downregulates the expression of corticotropin-releasing hormone (CRH) in the hypothalamic paraventricular nucleus and reduces c-Fos expression, a neuronal activation marker. The downstream result: less CRH means less adrenocorticotropic hormone, which means lower circulating cortisol. In a 2026 murine study by Lelong and colleagues, chronically stressed mice receiving R. rosea root powder standardized to 3% salidroside showed significantly reduced serum corticosterone and measurably less anxiety-like behavior compared to untreated stressed controls.
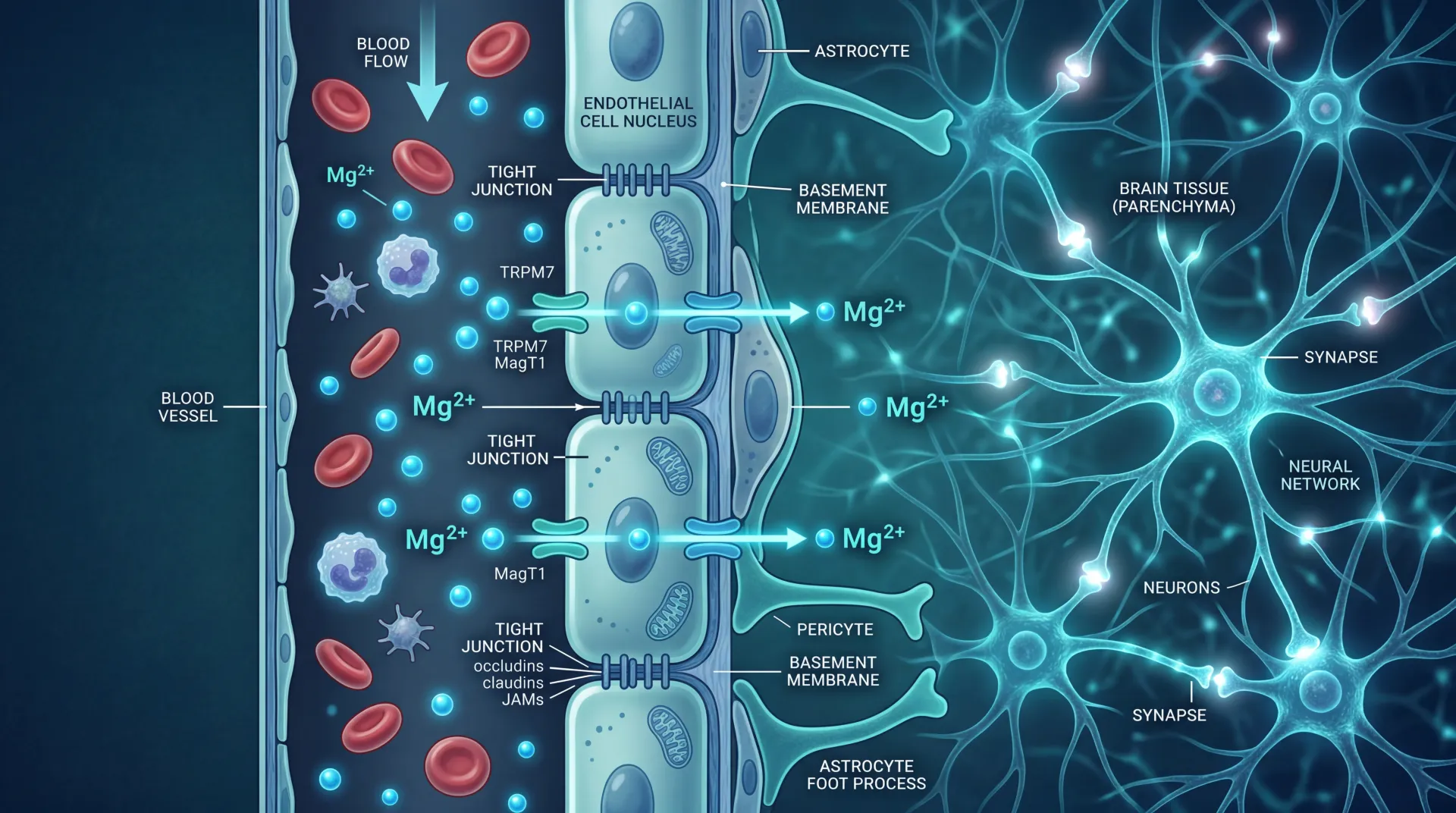
The story gets more complicated in the brain itself. R. rosea increases the permeability of the blood-brain barrier to precursors of dopamine and serotonin, which means raw materials for these neurotransmitters reach neurons more efficiently. It also inhibits monoamine oxidase A and B, the enzymes that break down serotonin, dopamine, and norepinephrine. That dual action, more precursors getting in and less neurotransmitter being destroyed, is the same general strategy that pharmaceutical antidepressants use, though through different molecular routes.
There is also a less-discussed pathway involving heat shock protein 70 (Hsp70). According to a review by Alexander Panossian, adaptogens like Rhodiola appear to upregulate Hsp70, a stress-sensor protein that inhibits nitric oxide synthase and interacts with glucocorticoid receptors. Lower nitric oxide during acute stress preserves ATP production, which may explain the subjective feeling of maintained energy under pressure. The Russian researcher Nikolai Lazarev coined the term "adaptogen" back in 1947 to describe substances that increase nonspecific resistance to stressors without disturbing normal physiology, and Rhodiola remains one of the few botanicals that still fits that definition under modern scrutiny.
So Rhodiola works through at least three overlapping channels: HPA axis modulation (cortisol regulation), neurotransmitter availability (serotonin and dopamine), and cellular stress defense (Hsp70 and antioxidant pathways). No single mechanism explains everything. That is part of why the plant remains difficult to study with the precision drug regulators want.
Physicians on Night Shift, Cadets Under Fire, and Burned-Out Office Workers
The fatigue research on Rhodiola starts in Soviet-era military labs, moves through Scandinavian university clinics, and lands in German primary care offices. That trajectory matters. The earliest positive results came from institutions with direct incentives to find performance enhancers.
The best-known early trial comes from Darbinyan and colleagues in 2000. They gave 56 physicians aged 24-35 a dose of 170mg of standardized SHR-5 extract during two-week night-shift rotations in a randomized, placebo-controlled, double-blind crossover design. The researchers measured a composite Fatigue Index covering associative thinking, attention, visual and auditory perception speed, and short-term memory. The Rhodiola group showed a statistically significant improvement, and when participants crossed over to placebo during the washout period, performance reverted to baseline. The crossover design is a strength here because each participant serves as their own control.
Scale matters, and a study of 56 physicians is not going to settle anything. The more interesting numbers come from larger trials. Shevtsov and colleagues tested 161 military cadets aged 19-21 with a single dose of either 370mg or 555mg of SHR-5, and found a pronounced anti-fatigue effect at both doses with no significant difference between them. That last detail is telling: more is not necessarily better with this plant.
Moving from acute doses to chronic supplementation, Edwards and colleagues ran an open-label study in 101 adults with self-reported life-stress symptoms, giving them 200mg twice daily for four weeks. Every measured variable, stress symptoms, fatigue, quality of life, mood, concentration, and functional impairment, improved significantly by week four. The limitation: no placebo group. Open-label designs cannot separate pharmacological effects from the considerable power of believing you are taking something helpful.

The burnout data is where Rhodiola starts to look genuinely useful. A non-interventional study across 128 German primary care practices enrolled 330 patients with burnout symptoms, including exhaustion, depression, insomnia, and declining performance. After eight weeks of R. rosea supplementation, researchers documented considerable alleviation with very good tolerability. A separate double-blind, placebo-controlled trial in 60 participants with diagnosed fatigue syndrome found that 576mg per day for four weeks decreased cortisol response to awakening stress and improved concentration. The cortisol measurement is significant because it provides an objective biomarker rather than relying solely on how people say they feel.
More recently, a 2025 randomized controlled trial by Alix-Fages and colleagues tested four days of Rhodiola supplementation in 18 young adults performing bench press and bench pull exercises under mental fatigue conditions. The cognitive and mental fatigue effects were trivial to small. But the physical performance data showed something different: Rhodiola was significantly superior to placebo for bench press repetitions and bench pull velocity under non-fatigued conditions. Out of 52 comparisons, 14 small effect sizes favored Rhodiola while only 3 favored placebo.
What does this mean for someone deciding whether to try it? The fatigue evidence is strongest for stress-related, burnout-type exhaustion rather than pure physical tiredness. If your fatigue comes from chronic work pressure, poor sleep, and the grinding accumulation of daily stress, the clinical data suggests Rhodiola may provide modest relief. If you are looking for a pre-workout stimulant, the evidence is thinner and less consistent.
Your Brain on Rhodiola: Promising Rats, Disappointing Humans
The cognitive story for Rhodiola splits sharply between animal models and human trials, and that gap deserves honest attention.
On the animal side, the data looks convincing. A 2018 systematic review and meta-analysis by Ma and colleagues examined 36 preclinical studies involving 836 animals and found that R. rosea significantly improved escape latency in Morris water maze tests (the standard measure of spatial learning in rodents, P < 0.05), increased time spent in target quadrants (a memory measure), and decreased errors in avoidance tests. The mechanisms identified across these studies include antioxidant activity, cholinergic regulation, anti-apoptosis, anti-inflammatory effects, and improved cerebral metabolism. Five of the 36 studies specifically used hypobaric hypoxia models, finding that Rhodiola protected against oxygen-deprivation-induced cognitive impairment.
The problem is that rodent brains are not human brains, and the translation from promising animal data to reliable clinical effects has been rough. The Alzheimer's Drug Discovery Foundation conducted an assessment and found that the quality of many clinical trials was suboptimal and none have directly tested whether Rhodiola can prevent age-related cognitive decline or dementia. In one well-conducted randomized controlled trial in male students aged 17-19, researchers found no improvement in cognitive scores after 20 days of supplementation. A double-blind crossover study with 18 healthy adults prescribed 3mg/kg of Rhodiola found no effects on mood or cognitive function.
There are a few bright spots. Jowko and colleagues tested 26 male physical education students with 600mg of R. rosea for four weeks and found improved psychomotor performance, specifically faster simple and choice reaction times. But physical performance did not change, and neither did hormone profiles. That pattern, small improvements in reaction speed without broader cognitive enhancement, appears repeatedly in the literature.
The neurotransmitter story from the mechanism section helps explain why cognitive effects are hard to pin down. R. rosea stimulates noradrenalin, serotonin, dopamine, and acetylcholine receptors in the central nervous system at small and medium doses. In theory, that should enhance alertness and processing speed. In practice, the effects are subtle enough that they often disappear into the noise of normal cognitive variation in healthy young adults who are not particularly impaired to begin with.
If you are already functioning at a normal cognitive level, Rhodiola is unlikely to make you noticeably sharper. Where it might help is when your cognitive performance has been degraded by stress, sleep loss, or sustained mental effort. The Darbinyan physician study and the Shevtsov cadet study both showed cognitive improvements specifically under fatigued conditions, not as a baseline enhancer. That distinction matters more than most supplement marketing acknowledges.
The Mountain Problem: Strong Tradition, Weak Evidence
Rhodiola's association with altitude is ancient and widespread. The plant grows naturally at high elevations across the Arctic, Central Asian mountains, and the Himalayas. Tibetan medicine has used it against altitude sickness for centuries. Russian mountaineers and cosmonauts reportedly took Rhodiola extracts, and the connection between an altitude-adapted plant and altitude performance has an intuitive appeal that is almost too neat.
The problem is that intuition and controlled evidence do not agree here. The only rigorous randomized controlled trial testing a Rhodiola species against altitude sickness produced a flat negative result. Chiu and colleagues conducted a double-blind, placebo-controlled crossover trial with 102 participants who ascended from 250 meters to 3,421 meters on Hehuan Mountain in Taiwan. Participants took 800mg per day of Rhodiola crenulata extract (standardized to 2.38% salidroside) for seven days before ascent and two days during mountaineering. The result: acute mountain sickness incidence was 60.8% in both the Rhodiola and placebo groups (adjusted odds ratio 1.02, 95% CI 0.69-1.52). Severe AMS was actually slightly higher in the Rhodiola group (35.3% vs. 29.4%), though not statistically significant.

There are important caveats. This trial used R. crenulata, not R. rosea, and the two species have different phytochemical profiles. R. crenulata contains salidroside and tyrosol but lacks the rosavins characteristic of R. rosea. Whether R. rosea itself would perform differently against altitude sickness has never been tested in a proper RCT. That is a gap in the literature, not evidence of absence.
What about altitude-related exercise performance? The data is indirect but more interesting. De Bock and colleagues found that acute R. rosea intake improved three of six endurance parameters, including time to exhaustion, oxygen uptake, and carbon dioxide output, in young healthy volunteers at sea level. Noreen and colleagues showed that acute Rhodiola ingestion decreased heart-rate response to submaximal exercise and improved endurance performance by reducing the perception of effort. At the cellular level, animal studies suggest R. rosea activates ATP synthesis and resynthesis in mitochondria after intense exercise.
None of these exercise studies were conducted at altitude. Connecting them to altitude performance requires a logical leap: if Rhodiola improves oxygen utilization and reduces perceived exertion at sea level, those mechanisms should matter more in oxygen-poor conditions. The preclinical data fits this logic, with five studies in Ma's meta-analysis using hypobaric hypoxia models showing cognitive protection. But a logical argument is not clinical proof.
If you are planning a trek to altitude, the evidence does not support replacing proven prophylaxis (gradual acclimatization or acetazolamide) with Rhodiola. It might be worth considering as a supplement alongside standard protocols, particularly for exercise tolerance, but anyone selling it as an altitude sickness preventive is outrunning the science.
500mg, 200mg, or 50mg? The Dosing Confusion and the Quality Gamble
Most clinical trials that showed positive results used extracts standardized to a minimum of 3% rosavins and 1% salidroside, mimicking the naturally occurring 3:1 ratio in R. rosea roots. The most-studied specific product is SHR-5, manufactured by the Swedish Herbal Institute and used in many of the trials cited throughout this article. That matters because when you buy a random bottle off Amazon, you are not necessarily getting what those researchers tested.
Dosing varies widely across the literature. According to Examine.com, daily preventative doses as low as 50mg have been reported effective for chronic fatigue prevention. Acute anti-stress usage falls in the 288-680mg range. And here is the critical detail: Rhodiola appears to follow a bell-curve dose response, meaning effectiveness may actually decline above 680mg. The Shevtsov cadet study confirmed this indirectly when 370mg and 555mg produced equivalent results.
| Context | Dose Range | Duration Studied | Key Finding |
|---|---|---|---|
| Daily fatigue prevention | 50-200mg | 20 days to 12 weeks | Reduced chronic fatigue markers |
| Acute stress/performance | 288-680mg | Single dose to 4 days | Improved reaction time, reduced perceived exertion |
| Burnout recovery | 400-576mg | 4-12 weeks | Reduced cortisol, improved concentration |
| Depression (mild-moderate) | 340-680mg | 6-12 weeks | Modest antidepressant effects, fewer side effects than sertraline |
The LD50 of dry R. rosea extract in rats is 3.36 g/kg, which scales to roughly 235 grams for a 70-kilogram human. Given that a typical dose is 600mg per day, the safety margin is enormous. The National Center for Complementary and Integrative Health (NCCIH) rates Rhodiola as "possibly safe" for up to 12 weeks, with reported side effects including dizziness, headache, insomnia, and dry mouth. After prolonged use of higher doses (1.5-2 grams), irritability and insomnia may develop.
Drug interactions deserve attention. Rhodiola may interact with CYP2D6 and CYP3A4 substrates and could have additive serotonergic effects when combined with antidepressant medications. If you are taking SSRIs, SNRIs, or MAOIs, talk to your doctor before adding Rhodiola. The NCCIH also notes a reported interaction with losartan, a blood pressure medication. Pregnant and breastfeeding women should avoid it entirely due to insufficient safety data.
For athletes wondering about regulatory status: Rhodiola rosea is not on the 2026 WADA prohibited substances list.
Now for the part that should genuinely concern you: what is actually in the bottle you buy. A 2026 analysis by Porwollik and Jafari tested ten commercially available R. rosea supplements in the United States using laboratory-grade chromatography. Rosavin content ranged from 0.01% to 3.08%. Salidroside ranged from 0.07% to 2.91%. Several products contained substantially less than their labels claimed, and one product showed an undisclosed likely addition of synthetic salidroside. All seven tested capsule products contained trace amounts of arsenic, cobalt, and lead, with two products showing notably elevated levels. Rhodiola supplements are also prone to adulteration with other Rhodiola species that lack rosavins entirely.
| What to Look For | Why It Matters |
|---|---|
| Standardized to 3% rosavins, 1% salidroside | Matches clinical trial formulations; confirms genuine R. rosea |
| Third-party testing (USP, NSF, ConsumerLab) | Independent verification of contents and contaminants |
| Species identified as R. rosea (not just "Rhodiola") | Other species have different active compound profiles |
| GMP-certified manufacturer | Reduces contamination and mislabeling risk |
The practical upshot: the quality gap between what researchers tested and what consumers can buy is large enough to make positive trial results partly irrelevant if you happen to get a weak or adulterated product.
The Uncomfortable Gap Between Popularity and Proof
Rhodiola rosea is not a scam. The clinical trials are real, the mechanisms are biologically plausible, and the safety profile is genuinely good. But a $3.4 billion U.S. market growing at 10% per year suggests a level of consumer confidence that the evidence has not earned.
The NCCIH is blunt: "There isn't enough reliable evidence to determine whether rhodiola or its components are useful for any health-related purpose." Most research in humans, they say, is of low-to-moderate quality. The Alzheimer's Drug Discovery Foundation landed in the same place, flagging suboptimal trial quality across the cognitive literature and zero studies testing long-term neuroprotective effects.
Here is what the critics are pointing at. Many of the positive trials have small sample sizes. The 56 physicians, the 40 students, the 60 burnout patients: these are pilot-scale studies that can detect large effects but miss subtler ones and are vulnerable to statistical flukes. The larger trials (161 cadets, 330 burnout patients, 101 life-stress participants) are more persuasive, but some of those used open-label or non-randomized designs.
The depression data illustrates the issue well. In Mao's phase II trial comparing R. rosea to sertraline, Rhodiola showed 1.4 times the odds of improvement versus placebo while sertraline showed 1.9 times. Rhodiola had significantly fewer side effects. That is a legitimate finding, but it also means Rhodiola performed worse than a first-line antidepressant, just with better tolerability. For someone choosing between the two, that tradeoff matters, but it is not the same as saying Rhodiola is an effective antidepressant.
There is also an ecological concern that rarely makes it into health articles. R. rosea was added to the CITES list of protected species in late 2022 because commercial demand was driving overharvesting from wild populations. The plant grows slowly at high altitudes and is difficult to cultivate at scale. If global demand continues to grow at current rates, supply pressure could further incentivize adulteration with cheaper, less-studied species.

And there is the cytotoxicity finding that deserves mention: R. rosea extract was cytotoxic to cultured primary cortical neurons at a concentration of 100 micrograms per milliliter. This is an in vitro finding and does not directly translate to oral supplementation at normal doses, but it does remind us that "natural" does not automatically mean "harmless at any concentration." The safety data for use beyond 12 weeks is thin.
What would change the picture? Large-scale, multi-center, placebo-controlled RCTs with 300+ participants, standardized extracts, and follow-up periods of six months or more. Studies specifically testing R. rosea (not R. crenulata) at altitude. Long-term safety data. And independent replication of the positive burnout and fatigue results by research groups without ties to supplement manufacturers. Until that evidence exists, Rhodiola remains a plausible but unproven intervention, better supported than most herbal supplements but still short of the bar that would make it a confident clinical recommendation.
Frequently Asked Questions
How long does Rhodiola rosea take to work?
Some clinical trials showed measurable effects from a single dose. In the Shevtsov military cadet study, a single dose of 370mg produced anti-fatigue effects within hours. For chronic conditions like burnout, the German primary care study documented noticeable improvements within one week, with continued improvement over eight weeks. The onset depends on whether you are using it acutely for performance or chronically for stress resilience.
Can I take Rhodiola rosea with antidepressants?
This requires medical supervision. Rhodiola inhibits MAO-A and MAO-B enzymes and may have additive serotonergic effects when combined with SSRIs, SNRIs, or MAOIs. While one clinical trial safely combined R. rosea with sertraline for 12 weeks, the broader interaction profile is not well characterized. Talk to your prescribing physician before combining them.
Is Rhodiola rosea the same as Rhodiola crenulata?
No. They are different species within the same genus. R. rosea contains rosavins (rosavin, rosin, rosarin), which are absent in R. crenulata. Most clinical research has been conducted on R. rosea, specifically the SHR-5 extract. R. crenulata is used in traditional Chinese medicine and was the species tested in the failed altitude sickness trial. Products labeled simply as "Rhodiola" without specifying the species may contain either one or a blend.
Does Rhodiola rosea help with weight loss?
There is no direct clinical evidence supporting Rhodiola for weight loss. Some animal studies suggest it may improve mitochondrial function and lipid metabolism during exercise, and its cortisol-lowering effects could theoretically address stress-related overeating. But no human trials have tested weight loss as a primary outcome, and extrapolating from cortisol mechanisms to weight management is speculative.
What is the best time of day to take Rhodiola?
Most clinical protocols administer Rhodiola in the morning or early in the day. Higher doses taken later in the day may cause insomnia in some people, consistent with the plant's mild stimulant properties. For acute performance benefits, studies have used doses 30-60 minutes before the target activity. For chronic use, morning dosing with food is standard.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.