
The Hormonal Cliff Your Hair Doesn't Survive
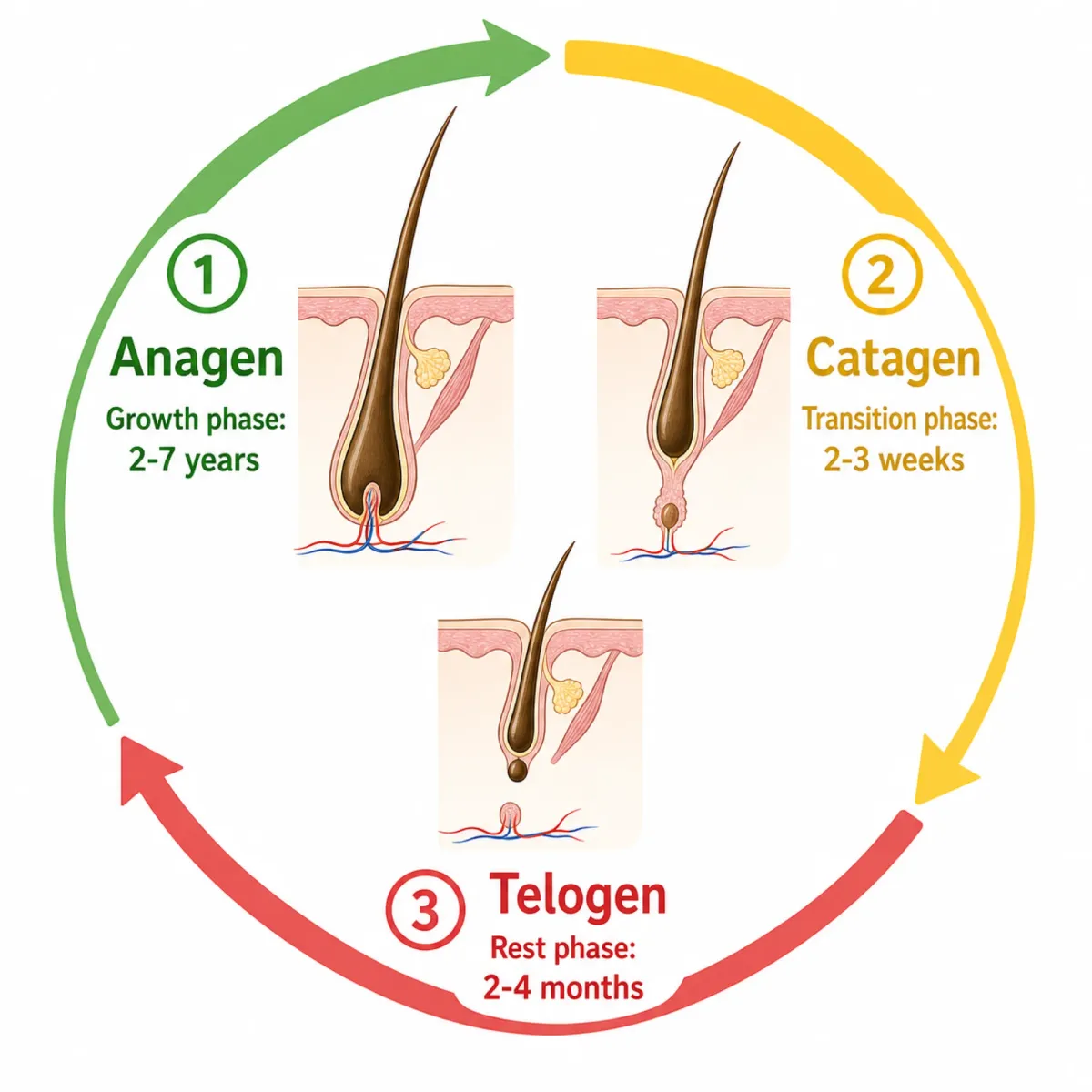
Picture your hair follicles as a factory floor running two shifts. During the growth phase (anagen), workers build new hair for roughly four years. Then comes the rest shift (telogen), about four months of dormancy before the cycle restarts. On a healthy scalp, around 85% of follicles are in the growth phase at any given time, with only 15% resting. That ratio keeps shedding to a manageable 80 to 100 hairs per day.
Pregnancy wrecks this orderly rotation.
During pregnancy, estrogen surges to roughly eight times its normal level while progesterone climbs ninefold. All that estrogen locks hair follicles into the growth phase, which is why many pregnant women notice their hair looking thicker and fuller than it has in years. The factory is running an extended shift with nobody clocking out.
Then delivery happens. Estrogen drops sharply after birth, and the hair follicles that were coasting on those elevated hormones suddenly enter the resting phase simultaneously. Instead of the usual 15% of follicles resting, a much larger percentage goes dormant at once. Two to five months later, when those follicles try to restart, the old hairs get pushed out in clumps. Handfuls in the shower. Enough on your pillow to make you wonder if something is seriously wrong.
This is telogen effluvium, and it has a terrible name for something that is essentially your body recalibrating after nine months of hormonal excess. The exact prevalence is unknown, but dermatologists consider it quite common; most adults will experience at least one episode of TE in their lifetime, and the postpartum period is one of the most frequent triggers.
What Six Months of Shedding Actually Looks Like
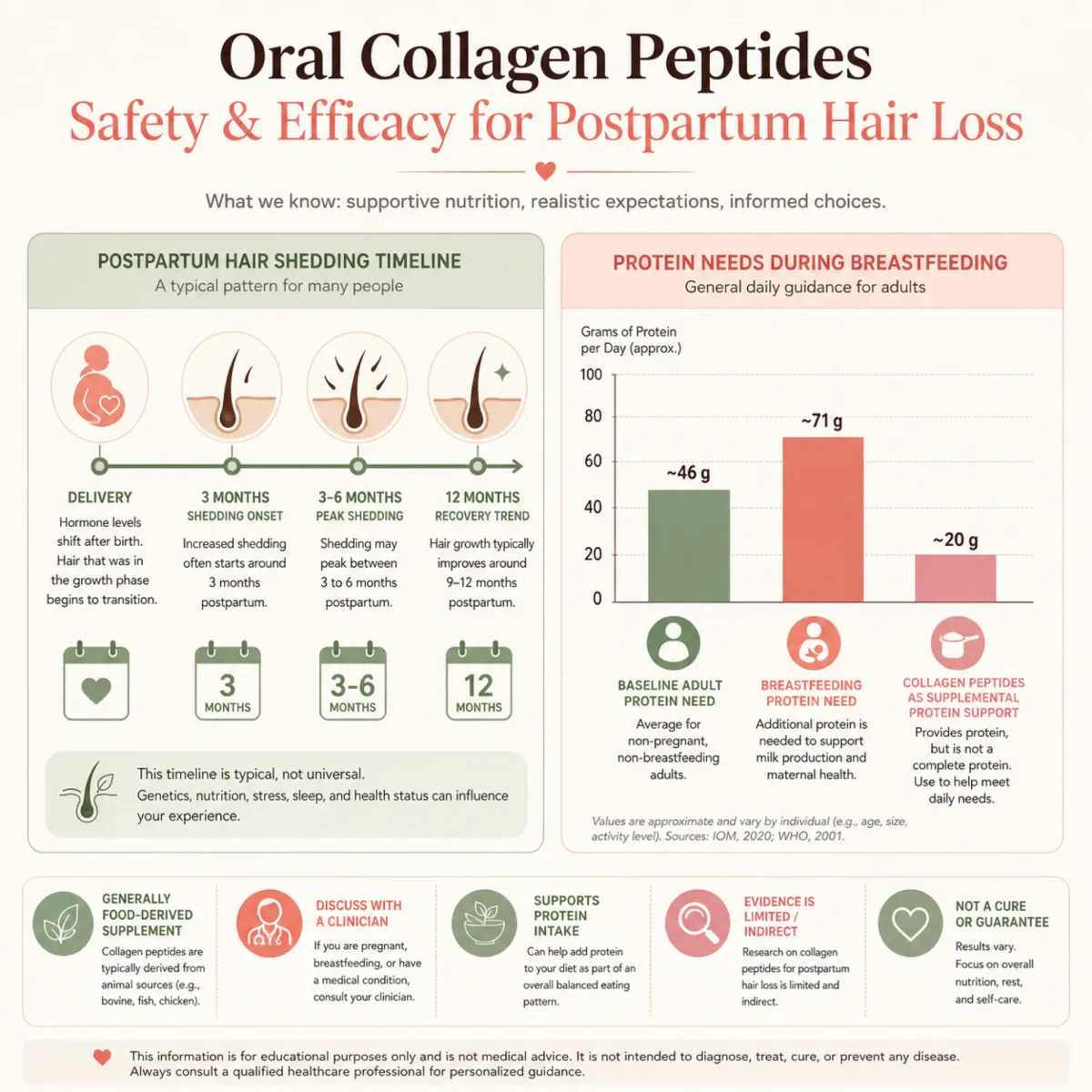
The timeline is both predictable and maddening. Hair loss typically begins about three months after delivery, though some women notice it as early as six weeks or as late as five months. The gap depends on individual hormonal dynamics and how quickly estrogen levels normalize, which according to research can happen within two to four days of delivery, even though the hair doesn't respond until weeks later.
What catches most new mothers off guard is the volume. You're not losing a few extra strands. Normal daily shedding is around 100 hairs from a scalp carrying 80,000 to 120,000. During postpartum TE, that number can double or triple. The shower drain fills faster. The ponytail holder wraps an extra loop.
The 6-12 month rule: Postpartum shedding typically peaks between months three and six, then gradually slows. Most women return to their pre-pregnancy hair density by their baby's first birthday. The condition is self-limiting, meaning it resolves on its own without treatment.
Acute telogen effluvium lasts less than six months in the vast majority of cases. If shedding continues past that mark, something else may be contributing, and that distinction matters for treatment decisions we'll cover later. But for the first six months, the single most evidence-based intervention is patience. Not a satisfying answer when you're watching your hair thin in real time, but it's the honest one.
That said, patience doesn't mean doing nothing. Several peptide-based approaches can support the recovery process, and they vary dramatically in both their evidence base and their safety profile for breastfeeding mothers.
Why Collagen Peptides Are the First Thing Worth Trying
Among every peptide category being marketed for hair growth, oral collagen peptides have something the others don't: a reasonable safety profile for postpartum and breastfeeding women. That's a low bar, but in a space where most compounds have zero lactation data, it matters.
Collagen is already abundant in your body. It's the scaffolding protein in skin, bones, tendons, and hair. Your hair is primarily made of keratin, and proline, one of the amino acids concentrated in collagen, serves as a direct building block for keratin production. The logic is straightforward: give the body more raw material for hair construction during a period when protein demands are elevated.
A 2016 study by Baginski and colleagues tracked women taking hydrolysed collagen protein from the third trimester through ten weeks postpartum and found the supplement safe and well-tolerated, with participants showing improved protein levels. It's not a large trial, and it wasn't designed to measure hair outcomes specifically, but it's one of the few studies that actually enrolled pregnant and postpartum women rather than extrapolating from general population data.
| Collagen Factor | Details |
|---|---|
| Breastfeeding safety | No known side effects reported |
| Recommended daily amount | 15 grams shown to increase collagen synthesis |
| Protein per 10g serving | Approximately 9 grams |
| Extra postpartum protein need | 17 additional grams daily (65-71g total) |
| Key limitation | Lacks tryptophan; not a complete protein |
The practical appeal extends beyond hair. Breastfeeding mothers need roughly 17 extra grams of protein daily, and many aren't hitting that target while managing a newborn. A collagen supplement contributes to the protein shortfall that's common during this period.
What collagen won't do is force dormant follicles back into growth. Collagen peptides have been shown to increase hair growth factors, but think of them as ensuring building supplies are on hand when follicles restart, not as a switch to turn them on early.
Topical Peptide Serums: What the Research Actually Shows
Dozens of peptide serums now target hair loss, and separating legitimate ingredients from marketing noise means looking at what's been tested in clinical settings versus what sounds impressive on a product page.
Three topical peptide compounds have the strongest evidence base, though "strongest" still comes with significant caveats.
Copper Peptide GHK-Cu
GHK-Cu is the most studied peptide for hair applications. Loren Pickart and Anna Margolina's research demonstrated that GHK-Cu can increase hair growth and thickness and enlarge hair follicle size. Their gene expression work showed the peptide affects 31.2% of human genes at 50% or greater change levels, which is a staggering breadth of biological activity for a single tripeptide.
The problem: no large-scale randomized controlled trials have demonstrated GHK-Cu's efficacy for hair regrowth in humans. The hair growth claims come primarily from preclinical models and small pilot studies. The mechanism is plausible. Controlled human proof is missing.
And for postpartum women specifically: GHK-Cu is listed as contraindicated during breastfeeding by multiple sources. Even in its topical form, the recommendation is to avoid it while nursing. Systemic absorption from scalp application is low, but without lactation safety data, the default recommendation from dermatologists is to wait until after weaning.
Biomimetic Peptide Serums (Redensyl, Procapil, Capixyl)
These compounds have been tested more directly for telogen effluvium. A double-blind placebo-controlled trial of Redensyl found that 85% of participants showed improvements, with a 9% increase in anagen hair and 17% decrease in telogen hair after three months. Procapil showed similarly encouraging numbers: an open-label study of 56 patients with androgenetic alopecia and telogen effluvium reported a 79% decrease in hair loss.
The most relevant study for postpartum women came from Dr. B.S. Chandrashekar's team at CUTIS Academy in Bengaluru, who compared three peptide serum formulations in 42 women with telogen effluvium over 90 days. The cytokine-based serum containing acetyl tetrapeptide-3 (the peptide backbone of Capixyl) alongside growth factors like IGF-1 and KGF performed best, achieving a 54.6% reduction in hair fall and a 6.16 percentage-point increase in anagen hair.
| Peptide Serum | Key Finding | Study Type | Limitation |
|---|---|---|---|
| Redensyl (3%) | 85% showed improvement; +9% anagen hair | Double-blind RCT (26 males) | Small sample, male-only |
| Procapil | 79% reported decreased hair loss | Open-label (56 patients) | No placebo control |
| Capixyl (acetyl tetrapeptide-3) | 46% increase in anagen/telogen ratio | Controlled (30 men, 4 months) | Small sample, male-only |
| Cytokine + peptide blend | 54.6% hair fall reduction in women with TE | Open-label (42 women, 90 days) | No placebo, single center |
No adverse events were reported across any of the three formulations in Chandrashekar's study, which is reassuring for tolerability. But none of these trials enrolled breastfeeding women specifically. The compounds are cosmetic-grade topicals rather than systemic medications, which puts them in a gray zone: probably lower risk than injectables, but without explicit lactation safety data, any dermatologist worth consulting will tell you to discuss it with your OB before starting.

The Case Against Injectable Peptides During Breastfeeding
BPC-157, thymosin beta-4, growth hormone secretagogues: if you've spent time in peptide communities, you've seen them recommended for everything from tendon repair to hair growth. Some have intriguing preclinical data. None belong in a postpartum protocol while you're breastfeeding.
Neither BPC-157 nor TB-500 has received FDA approval for human therapeutic use. They are not recognized as generally regarded as safe (GRAS) substances. The vast majority of available data for both compounds derives from animal studies, and the leap from rat models to human clinical confidence hasn't been made.
For postpartum mothers, the calculus gets worse. Pregnancy and lactation are explicit contraindications for BPC-157 and TB-500 due to the absence of safety data. The specific concern is blunt: the potential effects on fetal development and the unknown presence in breast milk make these peptides inappropriate for use during pregnancy or breastfeeding.
What "no safety data" actually means: It doesn't mean these peptides have been tested and found dangerous during breastfeeding. It means nobody has studied the question at all. There are no published pharmacokinetic studies on breast milk transfer for BPC-157, TB-500, or any growth hormone secretagogue. Zero. You'd be the experiment.
The same applies to growth hormone-releasing peptides like sermorelin, CJC-1295, and ipamorelin. These are systemic hormonal interventions that alter your GH axis. Whether those alterations transfer to breast milk or affect infant development is unknown.
| Peptide Category | FDA Approved | Human Hair Trials | Lactation Safety Data | Recommendation |
|---|---|---|---|---|
| Oral collagen peptides | GRAS (food protein) | Limited but positive | One study shows safety | Reasonable with OB approval |
| Topical serums (Redensyl, Procapil) | Cosmetic grade | Small positive trials | None specific | Discuss with dermatologist/OB |
| Topical GHK-Cu | Cosmetic grade | Preclinical only | Contraindicated | Wait until after weaning |
| Injectable BPC-157 / TB-500 | Not approved | None | Explicitly contraindicated | Do not use while breastfeeding |
| GH secretagogues (CJC-1295, etc.) | Not approved | None for hair | None | Do not use while breastfeeding |
If you've already weaned and the hair loss is persisting, the risk-benefit conversation with your doctor changes. But while you're nursing, injectable peptides for hair loss fail the most basic safety test: we don't know what they do to the baby. For a self-limiting cosmetic condition, that's not an acceptable trade.
Three Red Flags That Mean This Isn't Just Postpartum Shedding
Postpartum telogen effluvium resolves on its own. When it doesn't, the hair loss is usually postpartum TE sitting on top of something else. Knowing the difference can save you months of waiting for improvement that won't come without treating the real cause.
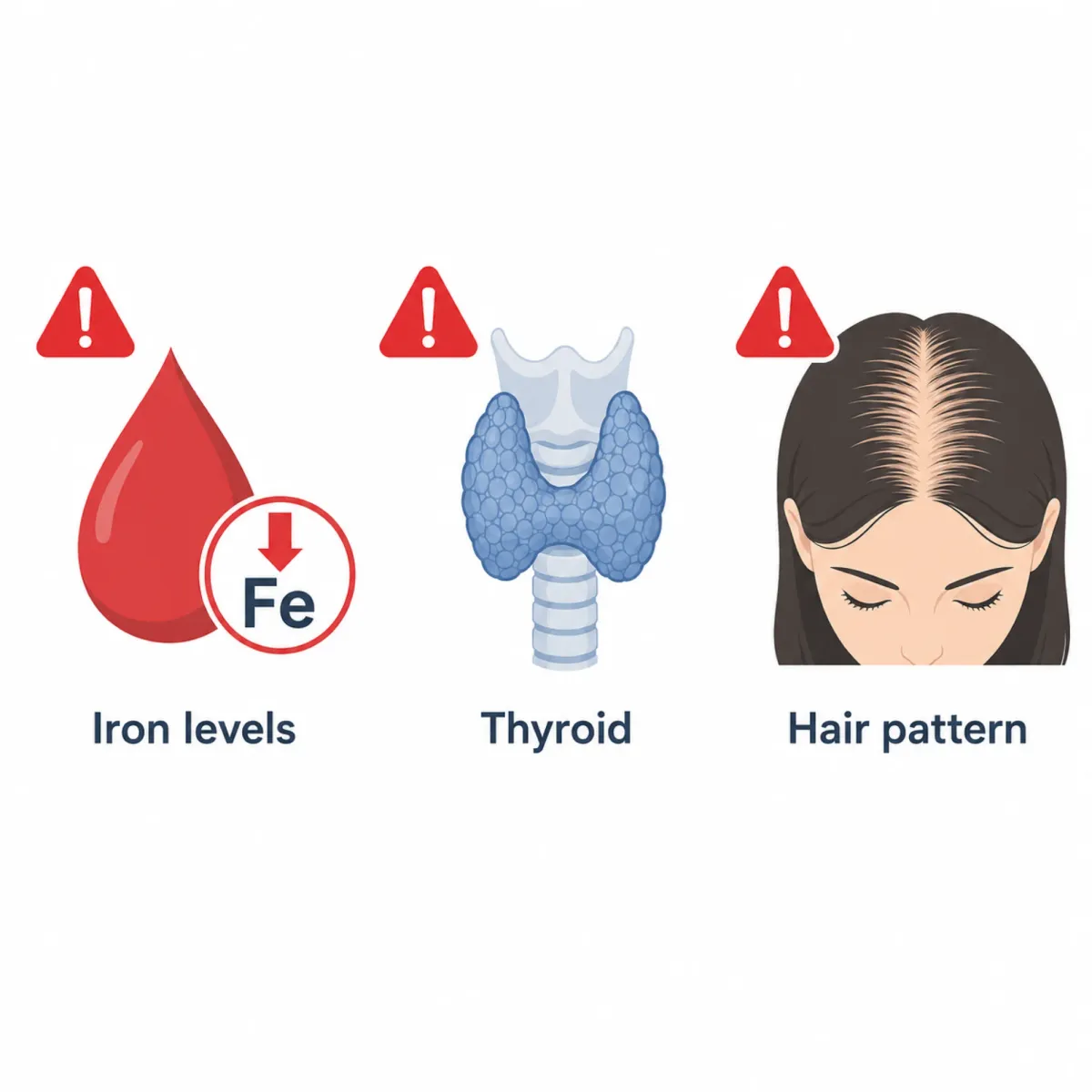
Red Flag #1: Iron Deficiency
This is the most common hidden driver and it's shockingly underdiagnosed. A study of 155 women with hair loss found that iron deficiency was the predominant cause in 70.3% of cases. Pregnancy and postpartum bleeding are among the top risk factors: obstetric and gynecological conditions accounted for 29.4% of the iron-deficiency alopecia cases studied.
The tricky part is the threshold. Standard blood work may show your hemoglobin is "normal," but adequate hair growth requires ferritin levels of 40 to 60 ng/mL, while the standard anemia cutoff of hemoglobin 12.0 g/dL corresponds to a ferritin of only 5.1 ng/mL. Your hair follicles can be iron-starved long before you'd be diagnosed as anemic. Ferritin proved a more sensitive marker than hemoglobin for early detection of iron deficiency related to hair loss.
Timing matters. Women who began iron supplementation within six months of hair loss onset had significantly better outcomes than those who waited longer. If your postpartum shedding seems excessive or isn't improving by month six, ask for a ferritin test specifically, not just a standard CBC.
Red Flag #2: Thyroid Dysfunction
Postpartum thyroiditis affects roughly 5-10% of women after delivery, and its symptoms overlap substantially with normal postpartum adjustment: fatigue, mood changes, and hair loss. A study of 500 women with telogen effluvium found that 30% had hypothyroidism and 20.4% had hyperthyroidism.
The hair loss severity difference was pronounced. Hypothyroid patients had mean hair loss severity scores of 44.2 compared to 25.6 for women with normal thyroid function, a statistically significant difference at P less than .001. Severe hair loss occurred in 34% of hypothyroid women compared to 18% of those with normal thyroid levels.
The researchers concluded that thyroid function testing should be included in the diagnostic workup for any patient presenting with telogen effluvium. This is doubly important in the postpartum period, when thyroid problems are more likely to develop and easier to miss.
Red Flag #3: Female Pattern Hair Loss Unmasked
Sometimes postpartum shedding reveals underlying androgenetic alopecia that was masked by pregnancy's hormonal boost. The telltale sign: instead of diffuse thinning everywhere, the part line widens or the crown thins more than the sides. This is a chronic, progressive condition with a different treatment pathway. Waiting for it to self-resolve won't work.
Frequently Asked Questions
Can I take collagen peptides while breastfeeding?
Oral collagen peptides are generally considered safe during breastfeeding, as collagen is a naturally occurring food protein. One clinical study tracked women taking hydrolysed collagen from late pregnancy through 10 weeks postpartum and found it safe and well-tolerated. However, always discuss any supplement with your OB or midwife before starting, especially if you have food allergies or sensitivities to the collagen source (bovine, marine, or poultry).
How long does postpartum hair loss actually last?
For most women, shedding peaks between months three and six after delivery and resolves by the baby's first birthday. If hair loss continues beyond six months or worsens after that point, it may indicate an underlying condition such as iron deficiency or thyroid dysfunction that needs separate evaluation.
Are injectable peptides like BPC-157 safe for hair loss while nursing?
No. BPC-157 and similar injectable peptides are explicitly contraindicated during lactation due to the complete absence of safety data. No studies have evaluated whether these compounds transfer into breast milk or affect infant development. For a self-limiting condition like postpartum telogen effluvium, the unknown risk to your baby is not justified.
Should I get my iron levels checked if my hair is falling out postpartum?
Yes, and specifically request a ferritin test rather than just a standard blood count. Research shows that adequate hair growth requires ferritin levels of 40-60 ng/mL, well above the threshold for clinical anemia diagnosis. Many postpartum women have ferritin levels low enough to affect hair growth without meeting the technical definition of anemia.
Do topical peptide serums work for postpartum hair loss specifically?
Clinical trials of topical peptide serums in women with telogen effluvium have shown hair fall reductions of 24-55% over 90 days. However, none of these trials enrolled breastfeeding women specifically. The serums are cosmetic-grade topicals with minimal systemic absorption, but discuss any topical treatment with your healthcare provider before use during breastfeeding.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.




