
Your Body Already Makes This Peptide. It Just Stops Making Enough.
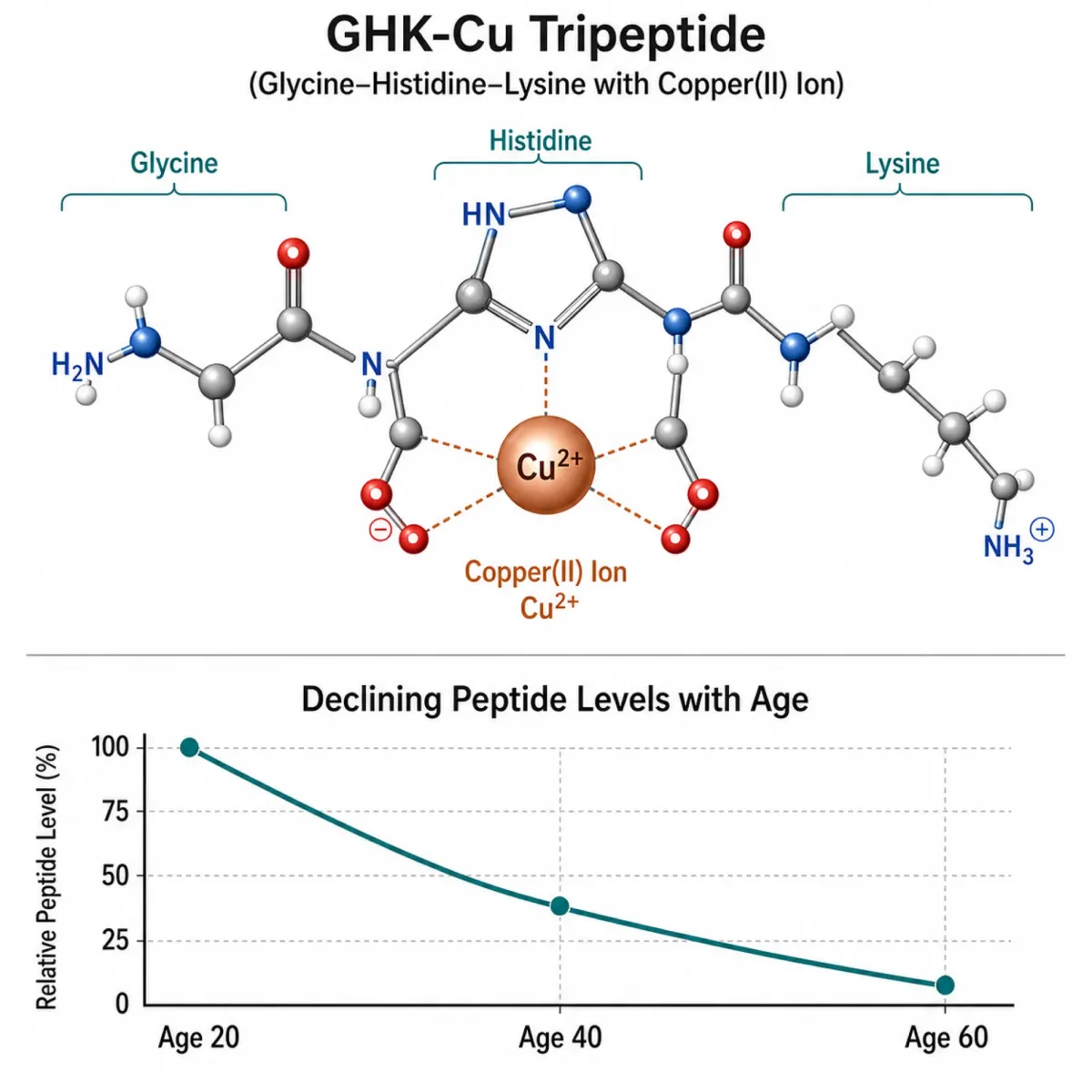
GHK-Cu is a tripeptide, three amino acids (glycine, histidine, lysine) bound to a copper ion. Your body produces it naturally. It circulates in blood plasma, shows up in saliva and urine, and plays a role in tissue repair throughout the body. None of this is new or controversial. What caught hair loss researchers' attention is what happens when you run out of it.
According to a 2018 review by Loren Pickart and Anna Margolina published in the International Journal of Molecular Sciences, circulating GHK-Cu levels sit around 200 nanograms per milliliter at age 20. By 60, that number drops to roughly 80 ng/mL. That 60% decline tracks uncomfortably well with the timeline of age-related hair thinning.
That same review produced a number that gets repeated across the peptide research world: GHK-Cu influences the expression of 31.2% of all human genes at a threshold of 50% or greater change. Of those affected genes, 59% get turned up and 41% get turned down. The analysis came from the Broad Institute's Connectivity Map, a drug-gene interaction database. Among the listed effects: increased hair growth and thickness, enlarged hair follicle size, boosted collagen synthesis (up to 70%), and suppression of TGF-β1, a protein implicated in pattern hair loss.
Think of GHK-Cu as something like a repair coordinator. It doesn't do one thing. It adjusts the settings on thousands of biological processes simultaneously. That's what makes it interesting for hair loss, and also what makes it difficult to study — when a compound touches 31% of your genome, isolating which specific pathway drives hair regrowth becomes a genuine scientific challenge.
One Signaling Pathway Controls Whether Your Follicles Grow or Quit
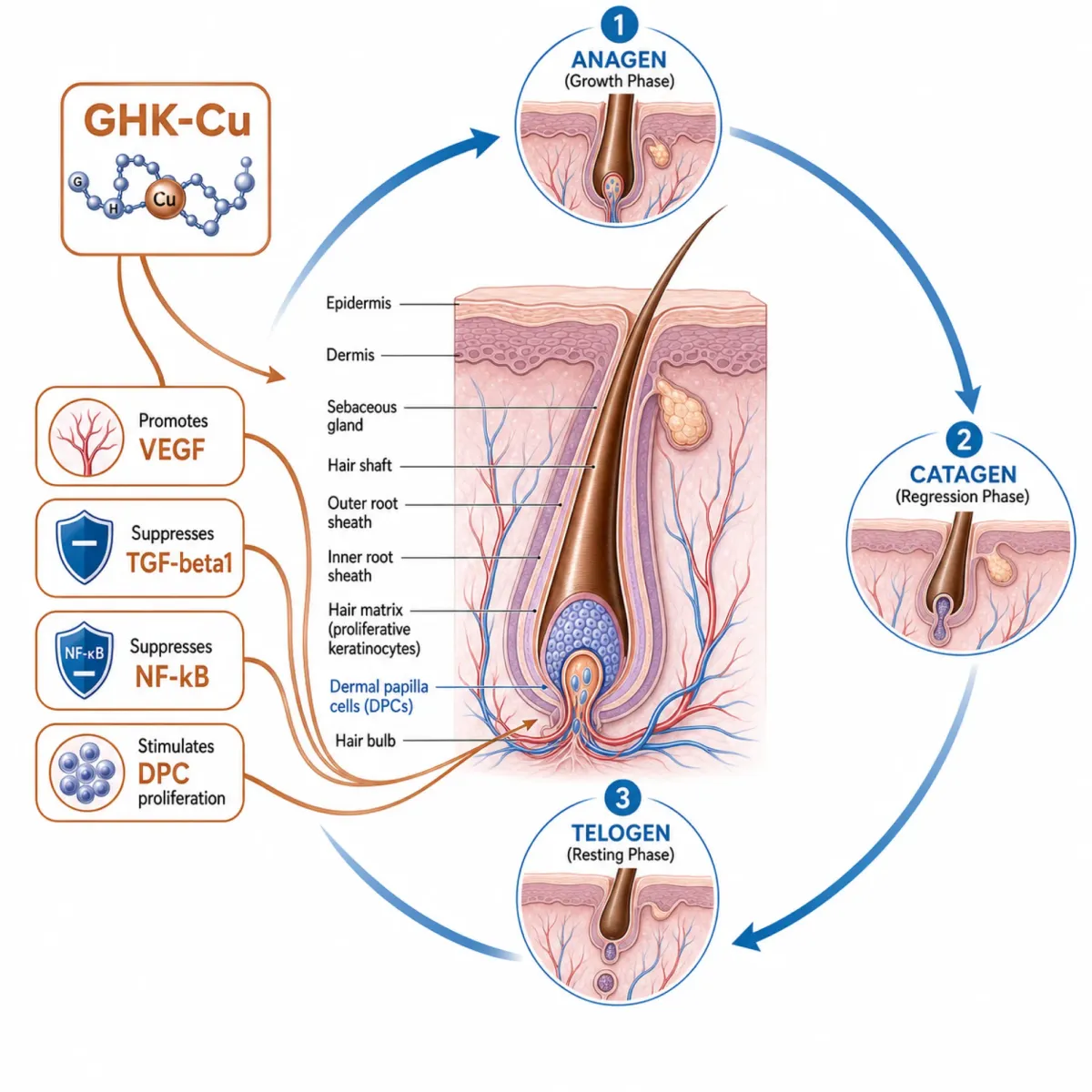
Hair follicles cycle through three phases: anagen (active growth, lasting 2-6 years), catagen (regression, a few weeks), and telogen (rest, 2-4 months). The switch between these phases depends on signals from dermal papilla cells (DPCs), a small cluster of specialized cells at the base of each follicle. Think of them as the growth command center.
The signaling pathway that matters most here is Wnt/β-catenin. A landmark 2010 study from Harvard Medical School by David Enshell-Seijffers and colleagues demonstrated exactly how central this pathway is. When they genetically deleted β-catenin specifically in dermal papilla cells, the results were dramatic: a 67% reduction in proliferating matrix cells (the cells that actually build the hair shaft), premature entry into catagen by four full days, and mutant hairs that grew to less than half their normal length.
The regeneration data was even more striking. Normal mice regrew a full coat within 20 days after depilation. The β-catenin-deleted mice produced no new hair coat even after 40 days. The follicle stem cells were still present and appeared normal — they just couldn't receive the "grow" signal from the dermal papilla.
The core mechanism is a feedback loop: keratinocytes (skin cells) release Wnt proteins that activate β-catenin in the dermal papilla, which then sends growth signals (FGF7, FGF10, Noggin) back to the matrix cells. Break this loop and the follicle stalls in telogen indefinitely.
A separate 2012 study confirmed this from the therapeutic angle: when researchers activated Wnt/β-catenin signaling in cultured human DPCs, the cells maintained their hair-inducing properties and successfully triggered new follicle formation when transplanted into mice. This pathway isn't just important for hair cycling — it determines whether dermal papilla cells retain their ability to initiate hair growth at all.
Where does GHK-Cu fit? The peptide works upstream and alongside this pathway rather than activating Wnt/β-catenin directly. Pickart and Margolina's gene expression data shows GHK-Cu suppresses TGF-β1 (a protein that drives follicle regression and fibrosis) and promotes VEGF production (building new blood vessels to feed follicles). It also suppresses NFκB signaling — the master regulator of inflammation that, when chronically activated in the scalp, contributes to follicle miniaturization.
A 2007 study from Seoul National University by Hyun Keol Pyo and colleagues tested copper peptides (AHK-Cu, a close analog) directly on human dermal papilla cells. At concentrations from picomolar to nanomolar ranges, the peptide stimulated DPC proliferation at statistically significant levels (p < 0.001) and reduced caspase-3 activity by 42.7% — caspase-3 being an enzyme that triggers programmed cell death. PARP cleavage, another apoptosis marker, dropped by 77.5%. In practical terms, the peptide was keeping dermal papilla cells alive longer and dividing faster.
One detail from Pyo's study that doesn't get enough attention: the dose-response curve was not linear. At higher concentrations (10⁻⁸ M), growth actually declined by 14.8%. At 10⁻⁷ M, it crashed by 81.5%. More copper peptide is not better. There's a sweet spot, and exceeding it reverses the benefit.
The Comparison Everyone Wants Has One Big Problem
No randomized controlled trial has ever compared pure GHK-Cu head-to-head against minoxidil for hair loss. That needs to be stated clearly because much of the online conversation treats this comparison as settled science. It isn't.
What we do have is indirect evidence from multiple angles. The closest thing to a direct clinical trial is Lee et al.'s 2016 randomized, double-blind, placebo-controlled study published in Annals of Dermatology. Forty-five men with pattern hair loss (Norwood-Hamilton II through V) used a topical spray containing GHK peptide combined with 5-aminolevulinic acid for six months. The low-dose group gained an average of 71.5 hairs per square centimeter. The high-dose group gained 52.6 hairs per cm². Placebo gained 9.6 (not statistically significant). Zero adverse events were reported across all three groups.
Those numbers look strong against typical minoxidil outcomes. But — and this matters — the active compound was a GHK + 5-ALA combination, not isolated GHK-Cu. You can't attribute the results to GHK alone.
| Factor | GHK-Cu | Minoxidil (2-5%) |
|---|---|---|
| Primary mechanism | Gene modulation, angiogenesis, anti-inflammatory, DPC stimulation | Vasodilation (widens existing blood vessels) |
| Hormonal effects | None documented | None (does not block DHT) |
| Common side effects | Rare mild redness | Scalp irritation, dryness, unwanted facial hair, headache |
| Dependency/rebound | Gains may reverse 3-6 months after stopping | Known rebound shedding on discontinuation |
| FDA approval for hair loss | No | Yes (OTC, both men and women) |
| Typical response rate | Not established in large trials | ~40% of men, ~25% of women show regrowth |
| Time to visible results | 3-6 months (anecdotal) | 3-6 months (clinical data) |
The mechanistic differences are real. Minoxidil is a vasodilator — it widens existing blood vessels to increase scalp blood flow. GHK-Cu promotes angiogenesis, which means it stimulates the formation of new capillaries rather than just dilating existing ones. It also reduces fibrinogen levels, improving microcirculation. Whether this translates to better hair outcomes hasn't been proven in head-to-head trials.
On safety, the comparison favors GHK-Cu more clearly. Minoxidil's side effect profile (scalp irritation, dryness, headache, occasional heart palpitations) is well-documented. Some users experience significant shedding when they stop using it. GHK-Cu, being a naturally occurring peptide, has decades of cosmetic use without reported adverse effects according to Pickart's review. The safety advantage is genuine even if the efficacy comparison remains incomplete.
Pyo's Seoul National University team, who studied copper peptide effects on dermal papilla cells, had previously used the same experimental model for minoxidil and found "similar proliferative and anti-apoptotic mechanisms" between the two. Pickart and Margolina's review characterized copper peptide effects as "comparable to 2% minoxidil" with a superior safety profile. Lab equivalence doesn't guarantee clinical equivalence, but it's enough to justify continued investigation.
3,000 Comments Can't Replace One Good Clinical Trial
A Reddit post on r/Biohackers titled "GHK-Cu before and after" collected over 1,600 upvotes and 603 comments. The poster described injecting 1mg subcutaneously every night, reporting reduced shedding and gradual hair improvements over months. Across r/tressless, r/HairlossResearch, and r/FemaleHairLoss, dozens of threads show a consistent vocabulary: "subtle," "gradual," visible only after three to six months. A four-month progress post described hair as "noticeably fuller, thicker, and holds shape a lot better."
Several patterns repeat across different users.
| Pattern | Frequency | Details |
|---|---|---|
| Skin improvements before hair | Very common | Users consistently report skin quality changes within weeks, while hair changes take months |
| Injectable outperforms topical for hair | Common | One user: "used topical versions for a year previously and noticed great skin results, but no hair improvements" — then saw temple regrowth with injectable |
| Shedding reduction first | Common | Decreased hair fall reported before visible new growth |
| AHK-Cu may beat GHK-Cu for hair | Recurring | "GHK-Cu on its own was more for scalp health and maintenance, while AHK-Cu gave the [better hair results]" |
| Temple/hairline regrowth | Occasional | Some report unexpected regrowth at temples, which is considered harder to treat |
| No hair benefit despite skin benefit | Occasional | Not everyone sees hair changes even with clear skin improvements |
The injectable vs. topical discrepancy is worth paying attention to. If subcutaneous injection works better for hair, that raises questions about whether topical GHK-Cu reaches the dermal papilla at sufficient concentrations. It also complicates the minoxidil comparison, since minoxidil was designed for topical scalp delivery.
None of this constitutes clinical evidence. Selection bias is extreme, placebo effect is uncontrolled, and protocol variations make comparison between anecdotes meaningless. But the consistency of certain patterns — skin-before-hair, injectable advantage — aligns with what the preclinical science would predict.

Why the Way You Apply It Might Matter More Than the Peptide Itself
Getting GHK-Cu to the dermal papilla is the central challenge. The papilla sits several millimeters deep in the dermis, below the epidermis and past the follicle's outer root sheath. Topical serums face a legitimate absorption barrier.
Microneedling has emerged as the most studied method for improving peptide delivery to follicles. A 2025 study published in JAAD International by Guilherme Kuceki and colleagues tested a professional-grade approach: five monthly sessions using a rotary tattoo machine with a 27-needle cartridge at 2mm depth, delivering a compounded solution of 0.5% minoxidil, 0.1% dutasteride, and 1.2% copper peptides. The results in seven men with Norwood-Hamilton Type III-IV hair loss: a median 26.5% improvement in Top Scalp Area Regrowth, with SALT severity scores dropping from 40% to 7.5% (p < 0.001).
The improvement over their previous 3-session protocol was substantial — 26.5% versus 10% TSAR (p = 0.0025). Zero adverse events across 35 total treatment sessions. The study referenced Dhurat et al.'s influential 2013 work showing that microneedling combined with minoxidil produced hair counts of 91.4 versus 22.2 for minoxidil alone — a fourfold difference from the physical delivery enhancement alone.
A critical caveat: Kuceki's study used a combination of three active ingredients (minoxidil + dutasteride + copper peptides), a professional-grade tattoo machine at 2mm depth, and dermatologist administration under local anesthesia. These results cannot be extrapolated to at-home dermarolling with a copper peptide serum.
For home use, the protocol is simpler: a 0.5mm derma roller used once weekly on clean, dry scalp, with copper peptide serum applied immediately after rolling. The channels stay open for roughly 15 minutes, bypassing the skin barrier. No shampooing for 12+ hours. Sterile, single-use rollers only.
A 2024 meta-analysis referenced in Kuceki's paper found combined microneedling therapy increased hair density by 13.36 to 18.11 hairs per square centimeter across pooled studies. Whether copper peptides add benefit beyond microneedling's own wound healing response is an open question — the micro-injuries alone trigger growth factor release (PDGF, VEGF, FGF) that could account for some results.
What the Current Evidence Supports If You Want to Try It
Concentration matters more than brand. Multiple sources converge on 0.5% to 2% GHK-Cu as the effective topical range for hair applications. Many commercial products market "copper peptide" formulas that contain less than 0.05% — well below the threshold where any effect has been documented. Check the actual percentage before purchasing.
The dose-response curve from Pyo's 2007 lab work offers a useful caution: copper peptides were effective at picomolar to nanomolar concentrations but inhibitory at higher levels. At 10⁻⁸ M, hair follicle growth declined 14.8%. At 10⁻⁷ M, it collapsed by 81.5%. This inverted U-shaped response means that more concentrated products are not automatically better and could theoretically work against you.
| Protocol Element | Recommendation | Notes |
|---|---|---|
| GHK-Cu concentration | 0.5-2% topical | Below 0.05% unlikely to work; above 2% not studied for safety at scale |
| Application frequency | Once daily (evening) | Some protocols suggest twice daily; data doesn't support one over the other |
| Microneedling depth | 0.5mm for home use | Professional settings use up to 2mm under anesthesia |
| Microneedling frequency | Once weekly | Apply serum immediately after needling while channels are open |
| Time to assess | Minimum 3-6 months | Shedding phase at weeks 3-6 is normal |
| Minoxidil stacking | Compatible but separate | Apply 20+ minutes apart; different pH ranges interfere with delivery |
| Finasteride stacking | Compatible | Different mechanisms (systemic DHT blocker vs. topical repair) |
Subtle improvements may appear at four to eight weeks, but noticeable thickness changes require three to six months. A shedding phase during weeks three through six is common and reflects follicle cycling reset rather than damage. Stopping during this window means absorbing the shed without reaching the regrowth payoff.
If stacking with minoxidil, don't apply both simultaneously — different pH ranges interfere with absorption. Separate by 20+ minutes or use morning/evening scheduling.
The data does not support expecting regrowth on completely smooth, bald scalp. GHK-Cu works on miniaturized follicles that are still present. Where the follicle has been destroyed, no topical peptide can rebuild it.

What the Enthusiasm Is Running Ahead Of
GHK-Cu has no FDA approval for hair loss. It has no large-scale randomized controlled trial for hair loss. The only RCT that exists (Lee et al., 45 subjects) tested a GHK + 5-ALA combination compound, not isolated GHK-Cu. Drawing conclusions about GHK-Cu's independent hair growth efficacy from that study requires assumptions the data doesn't support.
The bulk of the mechanistic evidence comes from Loren Pickart's body of work. Pickart's research is peer-reviewed and published in legitimate journals, but when one lab group dominates the published literature on a compound, that's a smaller evidence base than it appears. Independent replication from separate research teams is what turns promising findings into established science.
Specific gaps that matter:
- No head-to-head RCT against minoxidil. The comparison that would settle the debate doesn't exist. Lab data showing similar effects on dermal papilla cells is not the same as a clinical trial showing comparable regrowth on human scalps.
- Topical absorption is unquantified. We don't know how much GHK-Cu actually reaches the dermal papilla when applied to the scalp surface. The user review pattern (injectables working better than topicals for hair) suggests penetration may be a real limitation.
- Long-term safety data at therapeutic concentrations is thin. Cosmetic-grade products at low concentrations have decades of safety history. Higher concentrations (1-2%) applied daily to the scalp for years haven't been systematically tracked.
- Injectable GHK-Cu faces regulatory uncertainty. The FDA removed injectable GHK-Cu from its Category 2 list in April 2026, which affects compounding pharmacy access. This doesn't change anything about topical products (regulated as cosmetics), but it narrows the options for the delivery method that anecdotally works best.
- Combination confounders. Most positive studies use copper peptides combined with other active ingredients (5-ALA, minoxidil, dutasteride) or other procedures (microneedling, radiofrequency). Isolating GHK-Cu's contribution from these stacks is difficult to impossible.
The Kuceki microneedling study had seven participants and no control group. The Pamela 2021 study had three per group. These are pilot investigations useful for generating hypotheses, not proof of efficacy.
The honest assessment: the preclinical science is genuinely interesting, the safety profile for topical use appears favorable, and the cost is moderate. But the gap between what's published and what's claimed online is significant. Minoxidil has decades of large-scale trial data. GHK-Cu has mechanistic plausibility and early-stage results that justify optimism, but not confidence.
Frequently Asked Questions
Can GHK-Cu regrow hair on a completely bald scalp?
No. GHK-Cu works on miniaturized follicles still producing thinner, shorter hairs. Where follicles have been destroyed entirely, no topical treatment can rebuild them.
How long before I see hair results?
Expect three to six months of consistent daily use before visible improvements. A temporary shedding phase during weeks three through six is common as follicles reset. Skin changes appear faster (within weeks), which can be frustrating when hair is the goal.
Can I use GHK-Cu and minoxidil together?
Yes, but not simultaneously. Their different pH ranges interfere with absorption when mixed. Apply at separate times of day or wait at least 20 minutes between them. GHK-Cu is also compatible with finasteride.
Topical or injectable for hair loss?
User reports suggest injectable GHK-Cu produces better hair results, possibly because topical application struggles to reach the dermal papilla at effective concentrations. However, injectable GHK-Cu was removed from the FDA's Category 2 compounding list in April 2026, limiting access. Topical serums (0.5-2%) combined with weekly microneedling represent the most accessible approach.
What concentration should I look for?
Products with 0.5% to 2% GHK-Cu. Many marketed "copper peptide" formulations contain less than 0.05% — below documented effective thresholds. Lab research also shows excessively high concentrations inhibit growth (inverted U-shaped dose response), so more is not automatically better.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.




