
Why Female Pattern Hair Loss Plays by Different Rules
A man losing his hair can usually point to his temples. Women get something entirely different. Female pattern hair loss (FPHL) thins the hair diffusely across the top of the scalp while typically sparing the frontal hairline. You might first notice a widening part, or a ponytail that feels thinner than it did two years ago. There is no receding line to track.
FPHL affects roughly 32% of adult women, with prevalence jumping from about 8% in women aged 20 to 29 up to 68% in women over 60. The treatment options are narrower than what men have access to, partly because the biology is different. In men, DHT shrinks follicles and finasteride blocks it effectively. In women, many with FPHL have completely normal androgen levels. Standard-dose finasteride (1 mg) has proven ineffective for postmenopausal women in clinical trials. The hormonal, genetic, and environmental factors driving FPHL overlap with male pattern baldness but do not replicate it. Think of two rivers starting from the same mountain range that carve very different valleys.
That biological gap explains why trichologists have been looking at peptides: small signaling molecules that influence follicle behavior through mechanisms other than DHT blocking. Three peptide approaches have accumulated enough evidence for clinical integration, though the evidence levels vary. None are FDA-approved for hair loss.

The Ludwig Scale: Where You Are Determines What Works
Trichologists classify female hair loss using the Ludwig Scale: Grade I is visible thinning along the part line, Grade II is pronounced widening across the crown, and Grade III is near-complete loss of coverage on top. Your grade shapes which peptide treatments make sense, because a follicle that has merely slowed down responds differently than one that has shut down.
Diagnosis goes beyond eyeballing the part. Trichoscopy examines follicle-level detail. The clinical marker is hair shaft diameter variation exceeding 20% among neighboring follicles. When some hairs are thick and others threadlike in the same zone, that miniaturization pattern confirms FPHL rather than temporary shedding.
Peptides work on existing follicles by improving blood supply, reducing inflammation, and supporting the growth cycle. They perform best at Ludwig Grade I and II, where follicles are miniaturized but structurally intact. By Grade III, where follicles may be fibrosed, peptide therapy alone is less likely to produce visible regrowth. Trichologists at that stage combine peptides with surgical or device-based interventions.
| Ludwig Grade | What You See | Follicle Status | Peptide Response Potential |
|---|---|---|---|
| Grade I | Widening part, mild density loss | Miniaturizing but active | Highest; follicles most responsive to stimulation |
| Grade II | Visible scalp through hair at crown | Significant miniaturization | Moderate; may need combination approach |
| Grade III | Near-complete thinning on top | Many follicles fibrosed | Limited as standalone; adjunctive role |
GHK-Cu: The Copper Peptide With 30 Years of Hair Research Behind It
GHK-Cu (glycyl-L-histidyl-L-lysine copper) is a tripeptide that occurs naturally in human blood plasma. Your body already produces it. The problem is how much it declines with age: plasma levels run approximately 200 ng/mL at age 20 and drop to 80 ng/mL by age 60. That 60% decline coincides almost exactly with the age window when FPHL accelerates in most women.
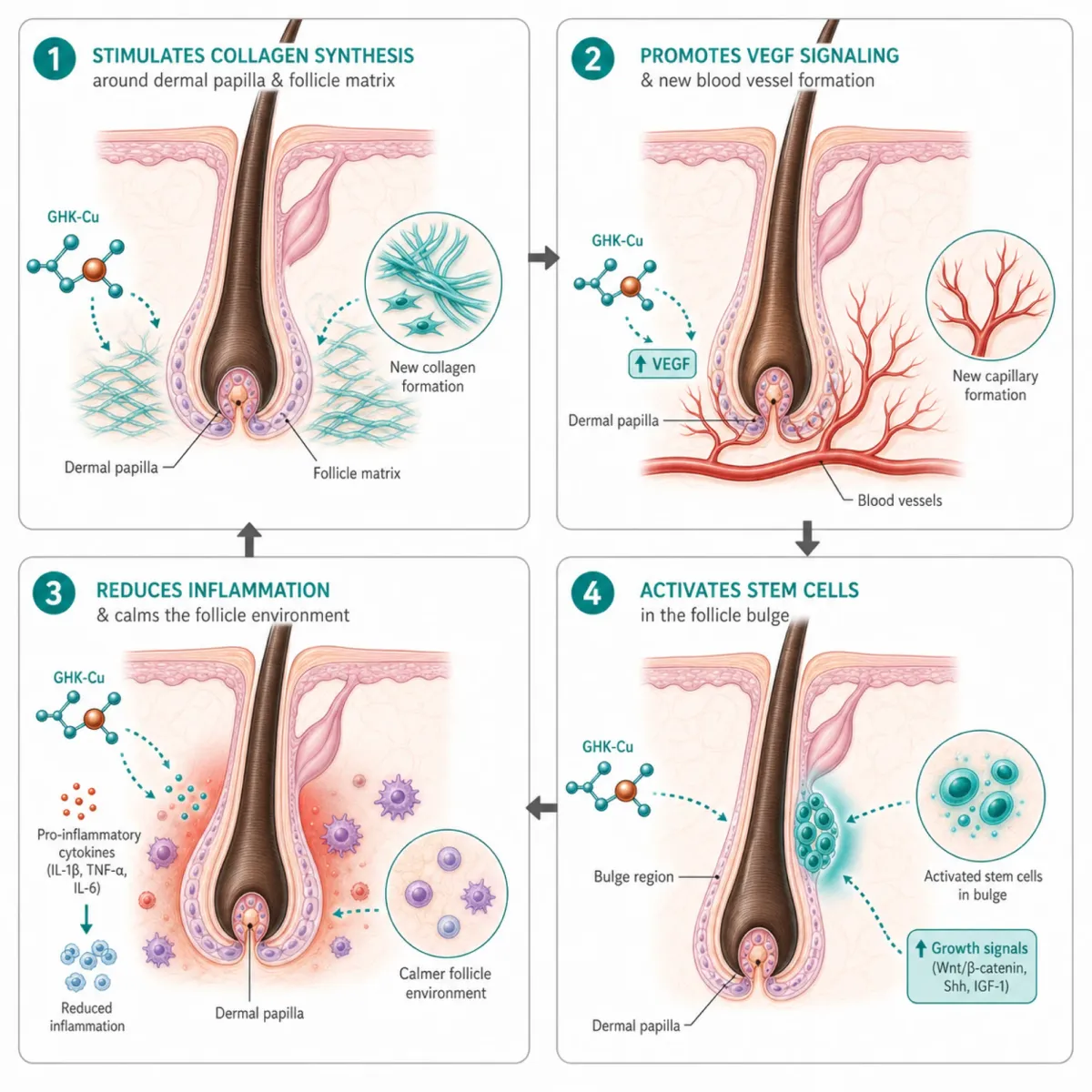
GHK-Cu's molecular reach is broad. Gene expression research found the peptide influences approximately 31% of human genes at a threshold of 50% or greater expression change. For hair, the relevant actions include stimulating collagen synthesis, increasing vascular endothelial growth factor (VEGF), and reducing inflammation via NFkB pathway modulation.
The strongest clinical data comes from a 2016 randomized, double-blind, placebo-controlled trial at Kyungpook National University in South Korea. Researchers tested a GHK complex (combined with 5-aminolevulinic acid) on 45 patients over six months. The low-dose group gained an average of 71.5 additional hairs per cm2, outperforming placebo by 7.4 times. The high-dose group saw 52.6 additional hairs. Zero adverse events across all participants. For context, topical minoxidil trials typically show gains of 12 to 25 hairs per cm2.
The study has important limitations. The sample was all male, the GHK was formulated with 5-ALA (so we cannot isolate GHK's contribution), and the biphasic dose response (lower dose working better) complicates dosing guidance. A separate 2025 study tested copper peptide delivery through microneedling-tattoo technique in seven treatment-resistant patients, achieving median scalp area regrowth of 26.5% with SALT scores dropping from 40% to 7.5% (P < .001). Small sample, male-only, but it shows copper peptides can contribute even when conventional treatments have failed.
GHK-Cu has been used in anti-aging products for decades without documented adverse effects. Trichologists typically prescribe it as a topical serum at 1% to 3% concentration, applied daily. For women who cannot tolerate minoxidil or who fall into the 30-60% non-responder bracket, GHK-Cu is a credible alternative with real research support.
Thymosin Beta-4: The Wound-Healing Peptide That Activates Hair Stem Cells
NIH researchers studying this 43-amino acid wound-healing peptide noticed something unplanned: treated animals consistently grew hair faster than untreated controls. That 2004 FASEB Journal finding launched a line of research that remains one of the more compelling threads in hair biology.
Thymosin beta-4 works at the stem cell level. Hair follicles contain stem cells in a region called the bulge. The NIH team found the peptide accelerated stem cell migration and differentiation at nanomolar concentrations while increasing MMP-2, an enzyme needed for extracellular matrix remodeling during growth. It operates through the Wnt/beta-catenin/Lef-1 signaling pathway, the same pathway controlling whether a follicle enters active growth (anagen) or resting (telogen). Transgenic mice overexpressing thymosin beta-4 regrew hair faster after shaving, while knockout mice showed dramatically reduced MMP-2 and VEGF levels.
The gap you need to know about: no human clinical trials have been published for thymosin beta-4 hair growth. Every positive result comes from rodents. Mouse follicle biology differs from human biology in ways that have sunk other promising compounds. Whether it works on human follicles, the optimal scalp delivery method, whether it can reverse androgenetic miniaturization, and its long-term safety profile all remain unresolved.
Thymosin beta-4 was restricted by the FDA in 2023-2024, limiting compounding pharmacy access. Its synthetic derivative TB-500 remains available through some clinics, though a March 2024 study questioned whether TB-500's benefits derive from its metabolite Ac-LKKTE rather than TB-500 itself. Trichologists who include thymosin beta-4 in protocols position it as experimental. The preclinical evidence is consistent, but prescribing it for women's hair loss requires honest disclosure that the evidence base is entirely animal-derived.
Biomimetic Peptides: Capixyl, Redensyl, and the Clinically Tested Alternatives
Biomimetic peptides are synthetic molecules designed to mimic naturally occurring growth signals. Three branded formulations dominate the OTC hair loss market: Capixyl, Redensyl, and Procapil. They are the peptide treatments women are most likely to find without a prescription. The clinical evidence behind them requires more scrutiny than most product pages provide.
Capixyl combines acetyl tetrapeptide-3 with biochanin A, a red clover extract that inhibits 5-alpha reductase locally. Biochanin A reduces DHT at the scalp without systemic hormone effects. A four-month study found Capixyl increased the anagen-to-telogen ratio by 46% versus a 33% decline in placebo. A 24-week trial comparing it to 3% minoxidil in 32 men and women showed comparable efficacy.
Redensyl targets stem cells through BCL2 activation and beta-catenin signaling. In clinical testing, 85% of participants showed improvements in hair cycle ratios. But a 2020 peer-reviewed study found Redensyl showed no statistical change in actual hair density versus placebo. It shifted the ratio of growing-to-resting hairs without adding measurable scalp coverage.
Procapil blends oleanolic acid, apigenin, and a glycine-histidine-lysine tripeptide. No human clinical trials have been published for Procapil in isolation.

A 2019 combined RCP study (106 participants, 24 weeks) reported the peptide group achieved 64.7% positive researcher assessment versus 25.5% for minoxidil. Those numbers look good until you examine the methodology: the study conducted no objective hair count measurements and ingredient concentrations were never disclosed. Every published study on these ingredients has been funded by manufacturers, with small samples and no independent replication.
Capixyl has the strongest evidence of the three, with the DHT-inhibition mechanism making particular sense for FPHL. The 2025 International Journal of Trichology review concluded these ingredients may find their place in patients who suffer adverse effects from standard therapies or as add-on treatments. For women who want to avoid or supplement minoxidil, Capixyl-containing serums are the most defensible choice in this category.
| Biomimetic Peptide | Key Mechanism | Strongest Clinical Finding | Evidence Limitation |
|---|---|---|---|
| Capixyl | Local DHT inhibition + ECM anchoring | 46% improvement in anagen/telogen ratio | Small, manufacturer-funded studies |
| Redensyl | Stem cell apoptosis reduction | 85% showed improvement in hair cycle ratios | No change in actual hair density vs placebo |
| Procapil | 5-alpha reductase inhibition | 67% improvement in anagen/telogen ratio (combined study) | Zero isolated human clinical trials |
How Peptide Treatments Compare to Minoxidil and Spironolactone
Topical minoxidil remains the treatment with the highest level of clinical evidence for FPHL, with a meta-analysis showing a mean increase of 12.4 hairs per cm2 after 24 weeks. But it has real problems for many women. Facial hypertrichosis occurs in 1.9% to 5.7% of users, and between 30% and 60% show no improvement. An estimated 60% of patients lack sufficient sulfotransferase enzyme to convert minoxidil to its active form in the scalp.
Spironolactone (100-200 mg daily, off-label) is the other mainstay, with over 70% of women reporting stabilization or improvement. Side effects include breast tenderness, menstrual irregularity, and hypotension, plus a pregnancy category X warning. Oral minoxidil at low doses has emerged as an alternative, producing 20 to 27 additional hairs per cm2, though hypertrichosis affected 54% of women in one study.
Peptides fill the gaps conventional treatments leave. A woman who gets facial hair growth from minoxidil and cannot tolerate spironolactone has limited options. GHK-Cu offers a topical alternative with no documented systemic side effects. Capixyl provides localized DHT inhibition without hormonal side effects. Thymosin beta-4 occupies the most experimental position, with compelling animal data but zero human hair-growth trials. No peptide matches the breadth of evidence behind minoxidil, which is why trichologists use them as part of multi-modal plans rather than standalone replacements.
| Treatment | Evidence Level | Density Gain | Non-Response Rate | Key Side Effect |
|---|---|---|---|---|
| Topical minoxidil 2% | High (multiple RCTs) | +12.4 hairs/cm2 | 30-60% | Facial hypertrichosis |
| Oral minoxidil 1mg | Moderate (RCTs) | +20-27 hairs/cm2 | Unknown | Hypertrichosis (54%) |
| Spironolactone | Moderate (retrospective) | 70%+ stabilization | ~30% | Breast tenderness, hypotension |
| GHK-Cu complex | Moderate (1 RCT, male) | +52-72 hairs/cm2 | Unknown | None reported |
| Capixyl | Low (small, manufacturer) | 46% ratio improvement | Unknown | None reported |
| Thymosin beta-4 | Preclinical only | Animal data only | N/A | FDA access restricted |
Building a Peptide Protocol: What Trichologists Actually Prescribe
Walk into a trichology clinic asking about peptides for FPHL, and the conversation starts with blood work, trichoscopy, and Ludwig Scale classification. Peptides are tools layered into a broader protocol, not first-line treatments.
A 2023 meta-analysis of 15 RCTs confirmed that combination therapies consistently outperformed monotherapy. In practice: minoxidil or spironolactone provides the base, peptides address specific gaps.
For Ludwig Grade I, GHK-Cu serum applied topically once daily is the most common peptide addition. Some clinics combine this with microneedling every four to six weeks, which independently showed density increases of 19.57 hairs per cm2 after three sessions. For Grade II, trichologists often add Capixyl-based serums alongside GHK-Cu, and may incorporate PRP injections (meta-analysis: density increases of 36.8 hairs per cm2, 95% CI 22.6-51.1) on a monthly-then-quarterly schedule.
Timeline expectations: Most peptide treatments require four to six months before visible results appear. Hair growth cycling means that new follicle activity initiated today will not produce visible length for several months. Trichologists typically schedule a six-month assessment to evaluate whether the protocol warrants continuation, adjustment, or a different approach.
GHK-Cu serums run $40 to $120 per month. Capixyl products are similarly priced. Thymosin beta-4 costs more when available through compounding pharmacies, with inconsistent access since the 2023 FDA restrictions. AGA is chronic, requiring lifelong maintenance therapy. Discontinuation leads to progressive hair loss within 12 to 24 weeks, so any protocol needs to be financially sustainable over years.

Peptides cannot rescue dead follicles. If surrounding tissue has fibrosed, no topical peptide will regenerate it. The window is while follicles are still alive but struggling. Early treatment at Ludwig Grade I maximizes the chance of shifting growth cycle balance before miniaturization becomes irreversible. Honest staging matters more than any specific product choice.
Frequently Asked Questions
Are peptide treatments for female hair loss FDA-approved?
No peptide treatment is currently FDA-approved specifically for hair loss in men or women. GHK-Cu has a long safety record in topical cosmetic products and one published RCT showing hair density improvements, but it is used off-label for hair loss. Thymosin beta-4 faces additional FDA restrictions enacted in 2023-2024 that limit compounding pharmacy access. Biomimetic peptides like Capixyl and Redensyl are sold in over-the-counter cosmetic products, which do not require FDA approval as drugs.
Can I use peptide hair treatments while on minoxidil or spironolactone?
Topical peptides like GHK-Cu and Capixyl are generally used alongside conventional treatments. The mechanisms differ enough that they should not interfere, and the clinical trend favors combination protocols. Spacing application times (minoxidil in the morning, peptide serum at night) helps ensure adequate absorption. Discuss any combination with your prescribing physician.
How long before I see results from peptide hair treatments?
Four to six months is the standard minimum timeline. Hair growth cycles mean that follicles stimulated today will not produce visible new length for several months. The 2016 GHK clinical trial showed progressive improvement through month six, with measurable gains appearing as early as month three. Trichologists typically assess progress at the six-month mark through repeat trichoscopy and standardized photography before deciding to continue, adjust, or change the protocol.
Is female pattern hair loss reversible with peptides?
FPHL is a progressive chronic condition. Peptide treatments can slow or partially reverse thinning when follicles are still structurally viable (Ludwig Grade I-II), but they do not cure the underlying condition. Discontinuing treatment typically leads to resumed progression within three to six months. Early intervention offers the best outcomes because it targets follicles while they are still capable of responding to growth signals.
What is the difference between GHK-Cu and the copper peptides in hair serums?
GHK-Cu is a specific tripeptide with a defined molecular structure and published clinical data. Some products label themselves as containing "copper peptides" without specifying the molecule or concentration. The hair growth research applies specifically to GHK-Cu. Look for that designation and a stated concentration of 1% or higher.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.




