
Roughly 40 percent of American adults have insulin resistance right now, according to research from Yale School of Medicine endocrinologist Gerald Shulman. Most of them do not know it. The condition rarely triggers obvious symptoms in its early stages, and doctors do not routinely test for it. By the time a blood panel catches something, the damage has often been accumulating for years.
That gap between onset and diagnosis is where this guide sits. Insulin resistance is not a mystery you need expensive lab work to unravel. Your body leaves clues in your waistline, your skin, your energy after meals, and your cravings. If you know what to look for and which numbers to track, you can catch it early and start reversing it before it progresses to prediabetes or type 2 diabetes.
What happens when insulin stops working
Insulin is a hormone your pancreas releases after you eat. Its job is to move glucose from your blood into your cells, where it gets burned for energy or stored as glycogen. When cells in your muscles, liver, and fat tissue stop responding to insulin properly, glucose builds up in your bloodstream. Your pancreas compensates by producing more insulin, a state called hyperinsulinemia.
This compensation works for a while. Your blood sugar looks normal on a standard test. But behind the scenes, your pancreas is working overtime, and elevated insulin is quietly doing damage: promoting fat storage around your organs, raising triglycerides, driving up blood pressure, and increasing chronic inflammation.
Gerald Shulman's lab at Yale has identified the core mechanism: fat accumulates inside liver and muscle cells where it does not belong (ectopic lipid), and those fat deposits disrupt the insulin signaling cascade. Shulman calls this an evolutionary adaptation hijacked by modern food. During periods of starvation, insulin resistance redirected scarce glucose to the brain. Now the same pathway gets triggered by caloric excess, and it stays on.
Insulin resistance can remain invisible on standard blood tests for 5 to 10 years before blood sugar rises enough to meet the threshold for prediabetes. By that point, the NIDDK estimates your risk of developing type 2 diabetes within the next decade is already high.
12 warning signs you can spot without a blood test
Insulin resistance is often called a "silent" condition, but it is not actually silent. It whispers. The problem is that the signals are diffuse and easy to attribute to aging, stress, or poor sleep. Here is what to watch for, organized by how early they tend to appear.
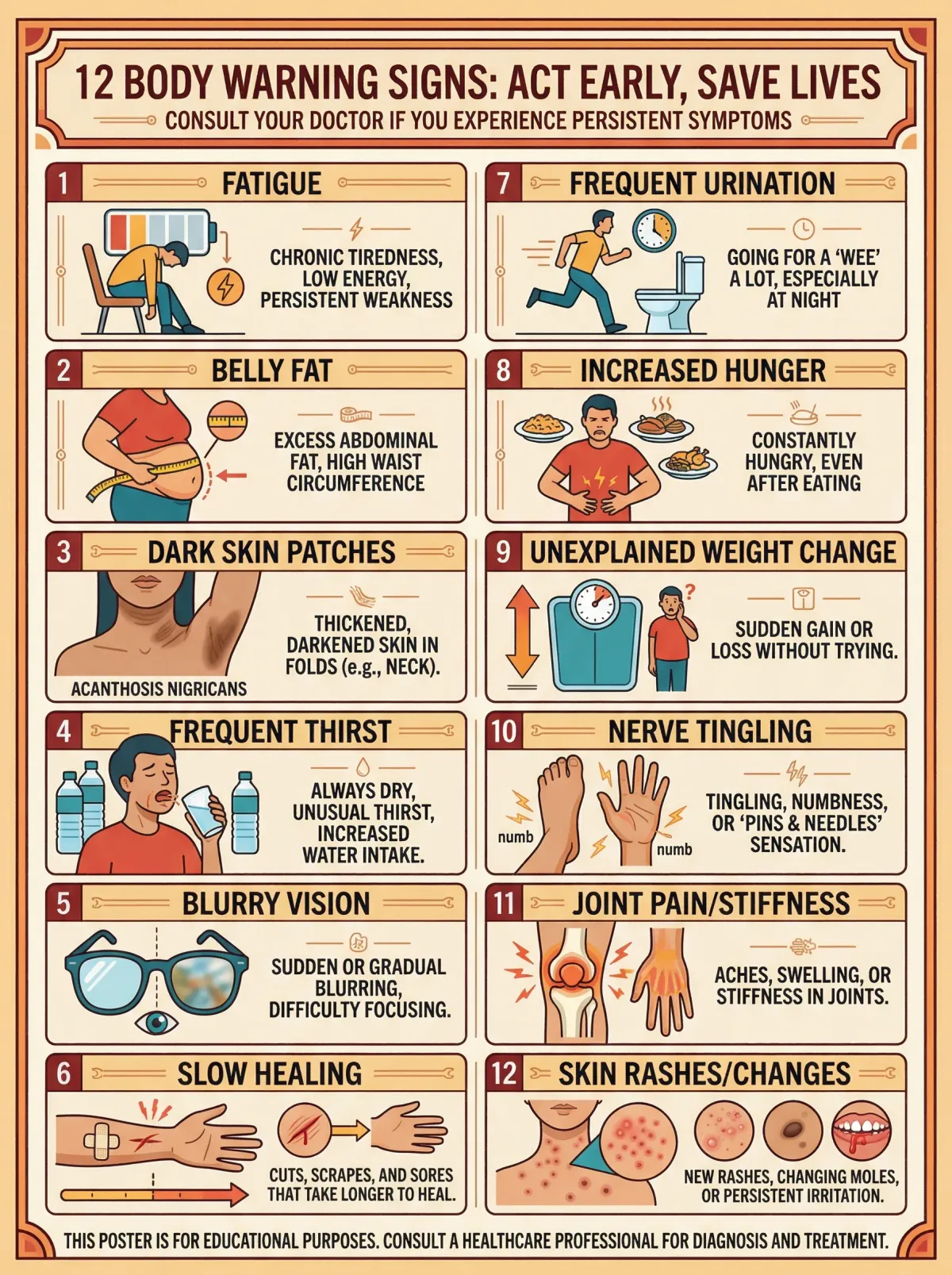
Early indicators
| Sign | What it looks like | Why it happens |
|---|---|---|
| Belly fat that won't budge | Expanding waistline despite effort | High insulin promotes visceral fat storage |
| Sugar cravings after meals | Wanting something sweet 30-60 min after eating | Cells not receiving glucose, brain signals hunger |
| Post-meal fatigue | Feeling sleepy or foggy after lunch or dinner | Blood sugar spike followed by crash as insulin overcompensates |
| Difficulty losing weight | Calorie restriction stops working | Elevated insulin blocks fat burning (lipolysis) |
Physical signs
| Sign | What it looks like | Why it happens |
|---|---|---|
| Acanthosis nigricans | Dark, velvety patches on neck, armpits, or groin | Excess insulin stimulates keratinocyte and fibroblast growth via IGF-1 receptor cross-reactivity |
| Skin tags | Small fleshy growths, often in skin folds | Linked to hyperinsulinemia and growth factor stimulation |
| Increasing waist circumference | Waist measurement creeping above 35 inches (women) or 40 inches (men) | Visceral fat accumulation driven by insulin |
Later-stage signals
| Sign | What it looks like | Why it happens |
|---|---|---|
| Persistent brain fog | Difficulty concentrating, mental sluggishness | Neuronal glucose uptake impaired; emerging Alzheimer's link |
| Frequent thirst and urination | Drinking more water, using the bathroom more often | Blood sugar beginning to exceed kidney reabsorption threshold |
| Hormonal irregularities | Irregular periods, worsening PCOS symptoms | Hyperinsulinemia drives excess androgen production in ovaries |
| Tingling in hands or feet | Numbness or pins-and-needles sensations | Early peripheral nerve damage from sustained high glucose |
A few of these on their own mean little. Three or four together, especially belly fat plus skin changes plus post-meal crashes, warrant investigation.
At-home measurements that actually matter
You do not need a doctor's appointment to start gathering data. Several well-validated measurements can be done in your bathroom with a tape measure and, optionally, an inexpensive glucose meter from the pharmacy.

Waist circumference
This single number is more predictive of metabolic risk than BMI. The metabolic syndrome criteria set the thresholds at 35 inches or greater for women and 40 inches or greater for men. Measure at the navel, first thing in the morning, before eating. Consistency matters more than a single reading, so track the number weekly.
Waist-to-hip ratio
Divide your waist measurement by your hip measurement (widest point around the buttocks). A ratio above 0.85 for women or 0.90 for men suggests central adiposity, the pattern most strongly linked to insulin resistance. This ratio catches people who carry visceral fat even if their overall weight seems normal.
Fasting blood glucose (at home)
A basic glucose meter costs under $30 and gives you a window into your metabolic health. Test first thing in the morning before eating or drinking anything besides water. According to the NIDDK, fasting glucose of 100 to 125 mg/dL falls in the prediabetic range. Below 100 is considered normal. Above 126 on two separate occasions points to diabetes.
Post-meal glucose response
Test your blood sugar 1 hour and 2 hours after eating a typical meal. Healthy levels return to under 140 mg/dL by the 2-hour mark. If you regularly see 140-199 mg/dL two hours after eating, that falls in the impaired glucose tolerance range that signals insulin resistance is already affecting how your body handles carbohydrates.
The metabolic syndrome checklist
The metabolic syndrome is often described as insulin resistance made visible through measurable markers. If you meet three or more of the following criteria, you likely have it:
| Marker | Threshold | At-home measurable? |
|---|---|---|
| Waist circumference | 35+ inches (women) / 40+ inches (men) | Yes |
| Fasting blood glucose | 100+ mg/dL | Yes (glucose meter) |
| Blood pressure | 130/85+ mmHg | Yes (home BP cuff) |
| HDL cholesterol | Below 50 mg/dL (women) / Below 40 mg/dL (men) | No (requires blood draw) |
| Triglycerides | 150+ mg/dL | No (requires blood draw) |
Three of the five markers can be checked at home. If you clear those three, you have strong reason to push your doctor for the remaining two on your next blood panel.
Why standard blood work misses early insulin resistance
Most annual physicals include a fasting glucose test and sometimes an A1C. Both measure blood sugar, not insulin. And that is the fundamental problem.
Insulin resistance begins years before blood sugar rises. Your pancreas can compensate for declining insulin sensitivity by pumping out more of the hormone. Blood glucose stays in the normal range, your doctor says everything looks fine, and the underlying resistance keeps building. The NIDDK acknowledges that health care professionals may not test for insulin resistance because the test is primarily used for research.
Even when insulin levels are measured, the results are hard to interpret. Research published in Current Opinion in Obstetrics and Gynecology found that HOMA-IR scores (the most common surrogate for insulin resistance, calculated from fasting glucose and insulin) showed greater than twofold variation depending on which insulin assay was used. The same person tested at two different labs could get meaningfully different results.
This does not mean blood work is useless. It means you should ask for the right tests and interpret them as a panel rather than isolated numbers. If your fasting glucose is creeping toward the mid-90s, your triglycerides are rising, your HDL is dropping, and your waistline is expanding, the pattern tells a story that any single number misses.
Request these specific tests at your next visit: fasting insulin (not just glucose), A1C, a full lipid panel with triglycerides, and fasting glucose. Look at the ratios. A triglyceride-to-HDL ratio above 3.0 is a strong independent predictor of insulin resistance.
Dietary shifts that restore insulin sensitivity
No supplement reverses insulin resistance on its own. Diet changes have more evidence behind them than anything else, and two factors matter: what you eat and when you eat it.

The Mediterranean pattern wins
The American Diabetes Association and Cleveland Clinic dietitians both recommend the Mediterranean diet for blood glucose management. The pattern emphasizes vegetables, whole grains, fish, legumes, nuts, and olive oil while limiting processed foods, refined carbohydrates, and saturated fats. It works because it addresses several insulin resistance drivers simultaneously: it lowers the glycemic load per meal, provides fiber that slows glucose absorption, and delivers omega-3 fatty acids that reduce inflammation.
Meal timing matters more than people realize
A Swedish study cited in the PMC literature found that people who ate regular meals had 60 to 70 percent lower odds of developing metabolic syndrome compared to irregular eaters, even after adjusting for physical activity. Eating at consistent times each day appears to stabilize the insulin response. Skipping breakfast and then overeating at dinner is one of the worst patterns for someone with insulin resistance.
The glycemic index as a practical tool
The glycemic index ranks foods by how rapidly they raise blood sugar. High-GI foods like white bread, potatoes, sugary cereals, and soda cause sharp spikes that demand large insulin responses. Low-GI foods like beans, berries, non-starchy vegetables, and whole grains produce gradual, manageable rises. You do not need to memorize a table. A useful rule: the more a food looks like it did when it came out of the ground, the lower its glycemic index tends to be.
Foods that help vs. foods that hurt
| Eat more | Eat less |
|---|---|
| Leafy greens, broccoli, cauliflower | White bread, white rice, pasta |
| Salmon, sardines, herring (omega-3s) | Fried foods, processed snacks |
| Beans, lentils, chickpeas | Soda, juice, sports drinks |
| Berries, apples, pears | Candy, cakes, pastries |
| Oats, quinoa, brown rice | Breakfast cereals, flavored yogurt |
| Nuts, seeds, olive oil | Saturated fats from processed meats |
Weight loss: how much is enough?
The NIH-funded Diabetes Prevention Program, one of the most cited studies in metabolic medicine, showed that losing just 5 to 7 percent of body weight reduced the risk of developing type 2 diabetes by 58 percent in high-risk individuals. Yale research goes further, showing that a 10 percent weight reduction can reverse liver insulin resistance. For a 200-pound person, that is 10 to 20 pounds, not the dramatic transformation people assume they need.
Caloric restriction does not need to be extreme. Shulman's research demonstrated that a modest reduction to roughly 1,200 calories per day significantly reduced liver fat and restored hepatic insulin sensitivity. The takeaway is not that 1,200 calories is the magic number, but that even moderate caloric reduction, if sustained, produces measurable metabolic improvement.
Movement patterns that pull glucose from your blood
Exercise does something unusual in insulin resistance: it sidesteps the problem entirely. According to Shulman, physical activity opens an alternative pathway for glucose transport into muscle cells, one that does not depend on insulin signaling at all. Muscles pull glucose from the blood whether insulin is working or not.
The benefit starts during the activity itself. A walk after dinner lowers blood sugar while you are walking. Over time, the effect compounds. Research cited by Cleveland Clinic found that light-intensity walking after a meal reduced both blood sugar and insulin levels. The body needed less insulin to manage glucose, which is improved insulin sensitivity by definition.
What works: the evidence-based prescription
The DPP study that produced the 58 percent risk reduction used a combination of dietary changes and 150 minutes per week of moderate-intensity physical activity, roughly 30 minutes five days a week. Cleveland Clinic recommends adding muscle-strengthening exercises twice weekly on top of that. Muscle tissue is a major glucose sink, and building more of it increases your baseline glucose disposal capacity. This is why resistance training has become a cornerstone of metabolic health advice, particularly for people over 40.
The post-meal walk
Walk for 10 to 15 minutes after your largest meal. Muscles contract, glucose gets pulled from the blood, and the post-meal spike that would otherwise demand a large insulin response gets blunted. A glucose meter will show you the difference on day one.
You do not need to train hard
Intensity matters less than consistency for insulin sensitivity. The DPP participants were not doing HIIT workouts or marathon training. They walked, swam, and cycled at a moderate pace. The data says 150 minutes per week at moderate intensity, which means you should be able to hold a conversation but feel slightly winded. If your current activity level is close to zero, even 60 minutes per week produces measurable improvement.

Sleep and stress: the underrated factors
Cortisol, the stress hormone, directly reduces insulin sensitivity. Short sleep duration and sleep disorders like sleep apnea are independently associated with insulin resistance, a connection documented across multiple studies referenced in the PMC literature. If you are exercising and eating well but sleeping five hours a night, you are fighting your own biology. Seven to eight hours of sleep is not optional for metabolic health. And stress management, whether through structured routines, meditation, or simply carving out downtime, supports the entire recovery process.
Frequently asked questions
Can insulin resistance be completely reversed?
In many cases, yes. The Diabetes Prevention Program demonstrated that lifestyle changes can prevent or delay progression to type 2 diabetes for at least 15 years. Cleveland Clinic states that insulin resistance is often reversible through diet, exercise, and weight management. The caveat is that genetic predisposition and certain medical conditions mean some people will always need to be more vigilant, but the metabolic markers (fasting glucose, triglycerides, waist circumference) can return to normal ranges with sustained effort.
How long does it take to see improvement?
Blood sugar improvements can appear within days of dietary changes and regular walking. Research from Yale showed that caloric restriction reduces liver fat and reverses hepatic insulin resistance relatively quickly. Most clinical studies measuring insulin sensitivity improvement use 8 to 12 week timeframes, and the DPP showed meaningful diabetes risk reduction within the first year. Measurable changes in waist circumference and fasting glucose typically appear within 4 to 8 weeks of consistent effort.
Should I ask my doctor for a fasting insulin test?
Yes, if you have risk factors. Fasting insulin provides earlier warning than fasting glucose because insulin rises first to compensate. However, insulin assays are not standardized across labs, and HOMA-IR calculations based on these numbers have known variability. The test is most useful as part of a panel alongside fasting glucose, A1C, triglycerides, and HDL. Present the pattern to your doctor rather than fixating on any single number.
Does berberine help with insulin resistance?
Some research supports berberine's ability to improve insulin sensitivity through activation of the AMPK pathway, the same pathway metformin targets. However, berberine is a supplement, not a replacement for dietary and exercise changes. Discuss it with your healthcare provider before starting, especially if you take other medications that affect blood sugar.
Is insulin resistance the same as prediabetes?
No, though they overlap. Insulin resistance is the underlying metabolic dysfunction. Prediabetes is a diagnostic category based on blood sugar thresholds (A1C 5.7-6.4% or fasting glucose 100-125 mg/dL). You can have insulin resistance for years before your blood sugar rises enough to meet prediabetes criteria. The NIDDK estimates that people with prediabetes have a high chance of developing type 2 diabetes within 5 to 10 years without intervention.
Related Articles
- Berberine for heart health and cholesterol - How this plant compound activates the same metabolic pathway as metformin and supports blood sugar regulation.
- Mediterranean diet for brain health and longevity - The eating pattern most consistently recommended for insulin sensitivity also protects your brain.
- Chronic inflammation and anti-inflammatory living - Insulin resistance and inflammation feed each other in a loop that diet and movement can break.
- PCOS natural management - Insulin resistance drives 65 to 70 percent of PCOS cases, making these two conditions deeply connected.
- Resistance training for women over 40 - Building muscle mass increases your body's capacity to dispose of glucose, making strength training a direct intervention for insulin resistance.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.

