
Between Mouth Tape and a 47-Step TikTok Routine, There Is an Actual Science of Sleep Optimization
Somewhere between "just go to bed earlier" and a 47-step TikTok routine involving mouth tape, nostril expanders, and two kiwis lies the actual practice of sleepmaxxing. Dr. Anita Shelgikar, director of the sleep medicine fellowship at the University of Michigan, describes it as "a collection of activities, products or hacks used simultaneously to optimize sleep quality and quantity." Dr. Sam Kashani, a sleep medicine specialist at UCLA, frames it more simply: a "modified or upgraded version of sleep hygiene."
The distinction matters. Sleep hygiene is the floor: keep the room dark, avoid caffeine late, maintain a consistent schedule. The American Academy of Sleep Medicine recommends at least seven hours per night for adults. Sleepmaxxing is what happens when you treat that floor as a starting point and ask what the science says about going further.
This guide skips the basics you already know. Instead, it covers five areas where emerging research offers real, measurable advantages: timing your body temperature drop, manipulating light exposure throughout the day, combining specific supplements that appear to work better together than alone, interpreting wearable sleep data without falling into the anxiety trap, and stitching all of it into a protocol that actually fits a real life.
The goal of sleepmaxxing is not perfection. Dr. Shelgikar warns that it "can backfire if it turns what should be a restorative process into a high-pressure chore." Keep that in the back of your mind as you read. The best sleep protocol is one you can sustain without stressing about it.
Your Body Drops 2 Degrees Every Night. Here's How to Work With It.
Your core body temperature hovers around 98.6°F during the day, but it does not stay there overnight. About two hours before you naturally fall asleep, your internal temperature begins dropping, and it continues falling until it bottoms out in the early morning hours. That decline is not a side effect of sleep. It is a trigger for it. The drop coincides with the release of melatonin, and the two processes reinforce each other. Think of your body temperature like a thermostat programmed to signal bedtime by dialing itself down. When you fight that signal with a warm room or the wrong timing, falling asleep takes longer and the sleep you get is shallower.
The Sleep Foundation recommends keeping your bedroom between 65 and 68°F (18.3-20°C), while experts quoted in Time magazine and CNN suggest ranges between 60 and 68°F. The variation reflects individual differences, but the direction is consistent: cooler is better for most adults. One exception worth noting: a 2025 Griffith University study published in BMC Medicine found that adults aged 65 and over showed reduced cardiac stress responses at 75°F (24°C), suggesting older adults may need warmer bedrooms than the standard recommendation.
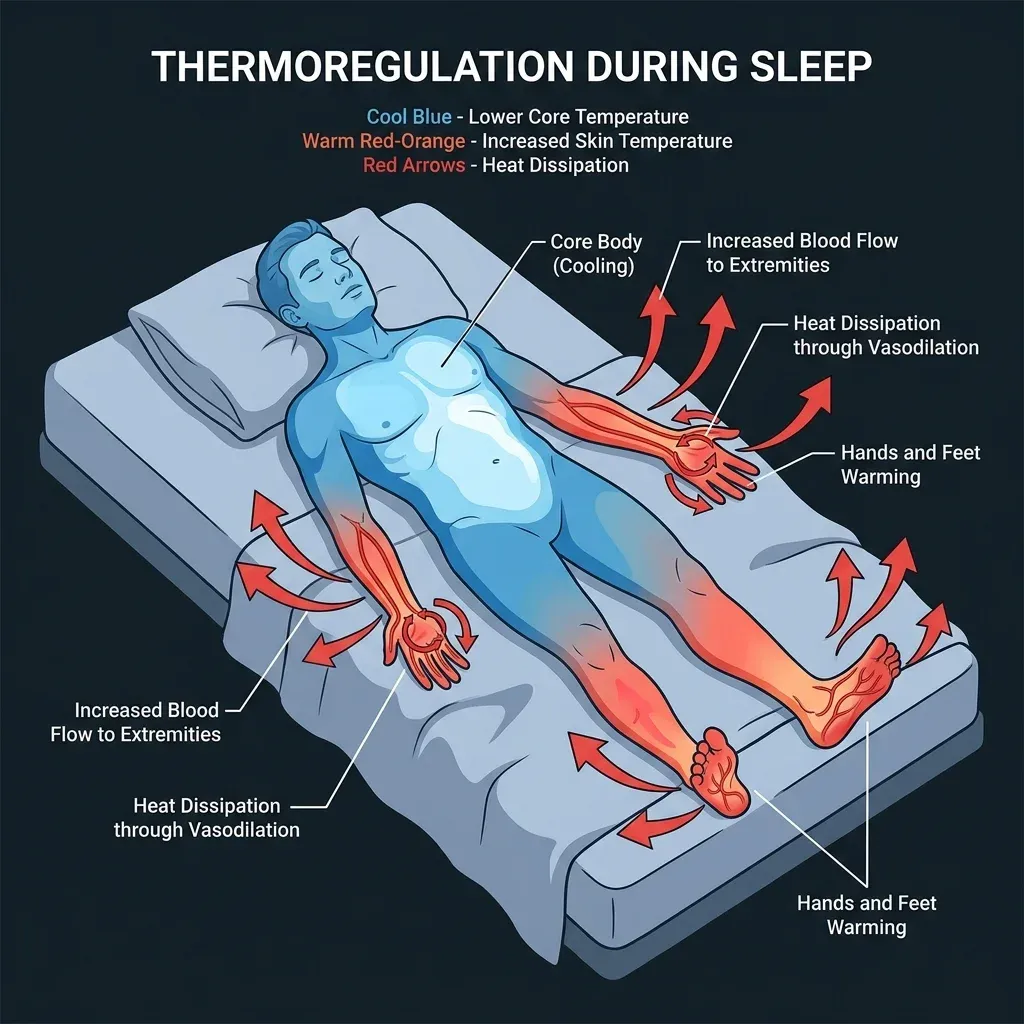
The mechanism behind all of this is vasodilation. Your circadian clock signals blood vessels in your hands and feet to open up, pushing warm blood to your extremities where heat can dissipate through the skin. This creates what researchers call the "distal-to-proximal skin temperature gradient" — your hands and feet warm up while your core cools down. If you have ever noticed warm feet right before you get drowsy, that is the process working correctly. People who have chronically cold feet may actually be at higher risk for sleep-onset insomnia because this heat-dissipation process is disrupted.
The warm bath trick, validated
A 2019 meta-analysis by Haghayegh et al., reviewing 17 studies (13 with quantitative data) from 5,322 candidate articles, found that a warm bath or shower at 104-108.5°F (40-42.5°C) taken one to two hours before bedtime significantly shortened sleep onset latency. The session needed to last just 10 minutes. The effect is counterintuitive — warm water raises your temperature temporarily, which then triggers an accelerated cooldown as blood rushes to the skin surface. You come out of the bath, your core temperature drops faster than it would naturally, and your body interprets that rapid decline as a stronger sleep signal.
The timing window matters more than most people realize. A bath three hours before bed may have worn off. A bath 30 minutes before bed may still have you warming up when you want to be cooling down. The one-to-two-hour window is when the rebound cooling aligns with your natural temperature dip.
| Temperature strategy | What to do | Why it works |
|---|---|---|
| Room temperature | Set thermostat to 65-68°F (60-67°F if you run warm) | Supports natural core cooling |
| Pre-bed warm bath | 104-108.5°F water, 10+ minutes, 1-2 hours before bed | Accelerates rebound core cooling |
| Cooling mattress/pad | Active cooling to ~67-70°F at mattress surface | Maintains cool microclimate all night |
| Warm socks | Wear socks if you have cold feet | Promotes vasodilation in feet for heat dissipation |
One thing the research does not always mention: what happens during REM sleep matters here too. During REM, your body largely stops thermoregulating — it will not sweat or shiver to adjust. That makes ambient room temperature especially important during the second half of the night when REM periods are longest. A room that felt fine at midnight might be disrupting your REM at 4 a.m. if it has warmed up.
The Lamp in Your Living Room May Be Sabotaging Your Sleep
Most sleep advice about light boils down to "avoid screens before bed." That is a starting point, but it misses the bigger picture. Your circadian system does not just react to the blue glow of your phone — it responds to every photon hitting your retina throughout the day, and the timing of those photons matters as much as their color.
The biology works like this: specialized cells in your retina called intrinsically photosensitive retinal ganglion cells (ipRGCs) contain a photopigment called melanopsin that is most sensitive to blue light in the 460-480 nanometer range. When these cells detect blue light in the evening, they signal the suprachiasmatic nucleus — your brain's master clock — to suppress melatonin production. Even short periods of evening screen use significantly reduce melatonin and delay its onset.
Your household lighting may be a bigger problem than your phone. A 2025 study published in Nature Scientific Reports tested 52 different lamps and found that cool white LED bulbs suppressed melatonin at a rate of 12.3% (measured by Melatonin Suppression Value), compared to just 1.5% for traditional incandescent bulbs — roughly eight times more suppression. Warm white LEDs came in at 3.6%, which is better but still double the incandescent rate. If you swapped your old incandescent bulbs for cool-white LEDs in the last few years, you inadvertently made your evening environment much more stimulating to your circadian system.
The tunable lamp solution
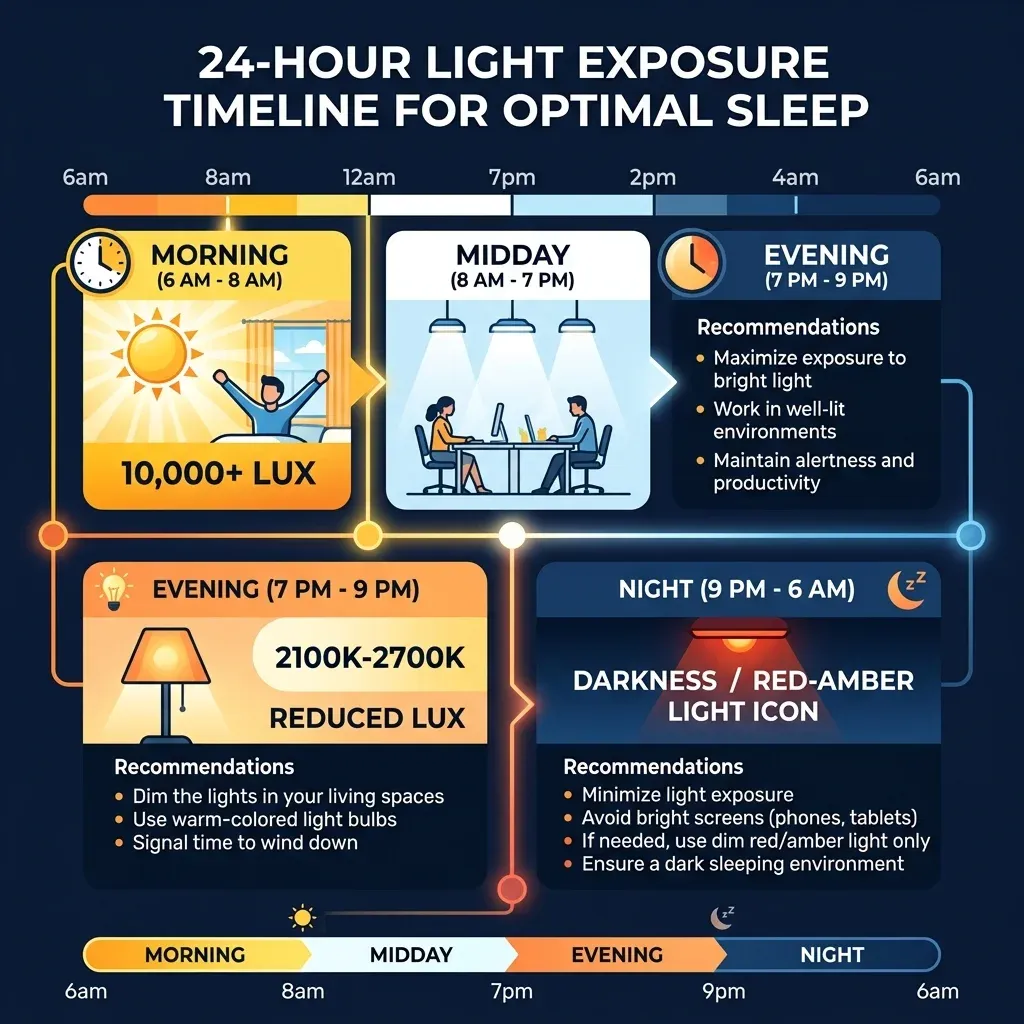
The same study found that tunable LED lamps could reduce estimated melatonin suppression from 10% at a cool 5700K setting down to just 0.1% at a warm 2100K setting. That is a 100-fold reduction by changing one setting. Smart bulbs from Philips Hue, LIFX, or even basic "warm dim" LEDs can achieve similar results. The practical move: program your evening lighting to shift from cool to warm starting around sunset, reaching its warmest setting by 8-9 PM.
Blue light blocking glasses: the nuanced reality
The blue-light blocking glasses market is enormous, but the research paints a complicated picture. A 2025 systematic review and meta-analysis of randomized controlled crossover trials by Luna-Rangel et al. found that blue-light blocking glasses produced a non-significant reduction in sleep onset latency of just 4.86 minutes (p=0.54) and a non-significant increase in total sleep time of 8.75 minutes (p=0.70). A Cochrane review reached similar conclusions: roughly half the trials showed benefits, while the other half did not.
The Nature lighting study helps explain why. Of eight blue-light filtering lenses tested, six produced only moderate effects — barely different from standard clear lenses. Only two lenses, both with a distinctly "brown" tint, reduced melatonin suppression below 0.3%. The cheap yellow-tinted glasses marketed as "blue blockers" may be filtering the wrong wavelengths or not filtering enough.
An interesting wrinkle comes from a 2025 Stanford-affiliated study of 39 schoolchildren: partial blue-light blocking glasses (40% cut) advanced sleep onset by about 10 minutes (p=0.041) and reduced daytime irritability, but they did not change salivary melatonin levels. The sleep benefit happened through some mechanism other than melatonin preservation, which researchers have not yet identified.
Morning light: the other half of the equation
Sleepmaxxing conversations focus almost entirely on what to avoid in the evening. But neuroscientist Dr. Andrew Huberman considers morning sunlight exposure one of the top five actions for physical and mental health. The protocol: get outside within the first hour or two of waking for 5-10 minutes on a sunny day, or 15-20 minutes on an overcast day. This triggers a cortisol pulse at the right time — early morning is when you want cortisol high — and sets the timer for melatonin release roughly 14-16 hours later.
A few rules that trip people up: regular eyeglasses and contacts are fine, but sunglasses block the relevant wavelengths. A car windshield or window also filters too much. And Dr. Samer Hattar, chief of the section on Light and Circadian Rhythms at the National Institute of Mental Health, has warned that bright screen use between 10 PM and 4 AM decreases dopamine levels and negatively affects mood, beyond just melatonin suppression.
Afternoon sunlight also matters. The yellow and orange wavelengths present when the sun is low create what Huberman calls a "second anchor point" for your circadian clock. It tells your brain that evening is approaching and begins the transition toward sleep. Even 10-15 minutes of late-afternoon outdoor light can partially offset the damage from artificial light later that night.

What a Mouse Study Revealed About Combining Two Common Supplements
The "Huberman sleep stack" — magnesium glycinate, apigenin, and theanine — has become one of the most widely discussed supplement combinations in the sleep optimization world. The evidence behind the individual ingredients is a mixed bag. The evidence behind combining two of them is surprisingly interesting, with one major caveat.
Start with the individual ingredients. Dr. James Rowley, a sleep specialist and professor of medicine at Rush University, says flatly that there is "no good evidence that magnesium is a reliable sleep aid" for people who are not deficient. Dr. Shelgikar adds that some medical conditions can worsen with magnesium supplementation. These are not fringe opinions. They reflect what the clinical literature actually shows for magnesium alone.
Apigenin, a flavonoid found abundantly in chamomile, has its own modest track record. According to a 2024 review in Frontiers in Nutrition by Kramer and Johnson, chamomile extract (which contains about 1% apigenin by weight) showed only a trend toward improvement in a 28-day insomnia trial — it did not reach statistical significance. A large cross-sectional study did find that low dietary apigenin intake correlated with worse sleep quality, but correlation is not causation. The reviewers themselves note it is "difficult to be certain whether the effects observed from chamomile extract are solely due to apigenin, other components of chamomile, or a combination of both."
The combination changes things — in mice
A 2026 study published in Food & Function (Royal Society of Chemistry) by researchers at Hong Kong Polytechnic University tested magnesium and apigenin separately and together across multiple mouse models. Neither supplement alone produced significant sleep improvement. But the combination increased sleep duration by 44% in normal mice (p<0.01), 32% in caffeine-disrupted mice (p<0.001), and 37% in a chemically-induced insomnia model (p<0.05). Those are not small numbers. And critically, the researchers used Bliss independence analysis to confirm the effect was genuinely synergistic — the combination did more than what you would predict by adding the individual effects together.
The mechanism makes biological sense. Apigenin acts on the GABAA receptor — the same target that benzodiazepines hit, though at a different binding site and much more gently. Magnesium regulates GABA neurotransmitter levels and is involved in melatonin synthesis through the enzyme N-acetyltransferase. Think of it as apigenin making the lock more responsive while magnesium helps produce the key. Together, they also suppressed inflammatory markers TNF-alpha (37%), IL-1 beta (31%), and IL-6 (23%) in the insomnia model — relevant because chronic sleep disruption and inflammation feed each other in a vicious cycle.
| Supplement | Mechanism | Evidence strength | Typical dose |
|---|---|---|---|
| Magnesium glycinate | GABA regulation, melatonin synthesis support | Weak alone (no strong RCTs for sleep) | 200-400mg elemental Mg, 30-60 min before bed |
| Apigenin | GABAA receptor modulation, anti-inflammatory, NAD+ boost via CD38 inhibition | Moderate (animal data strong, human chamomile trials mixed) | 50mg, 30-60 min before bed |
| Combination | Synergistic GABA + anti-inflammatory effects | Strong in mice, no human trials yet | Both at above doses |
The caveat cannot be overstated: this is a mouse study. No human clinical trial has tested the magnesium-apigenin combination. Mouse sleep physiology has meaningful differences from human sleep. The 44% improvement in mouse sleep duration should not be extrapolated to humans at any specific ratio. What the study does provide is a mechanistic rationale for why these two supplements, which individually show weak effects, might perform better together. If you are going to try a supplement stack for sleep, this combination at least has a plausible biological basis — which is more than can be said for most sleep supplements on the market.
Your Sleep Tracker Is 85% Right About Whether You're Asleep. It Guesses Your Sleep Stage Correctly About Half the Time.
Consumer sleep trackers have become central to sleepmaxxing culture. Oura Ring, Apple Watch, Whoop, and Samsung Galaxy Ring all promise to decode your sleep architecture — telling you how much deep sleep, REM, and light sleep you got, plus metrics like heart rate variability (HRV) and respiratory rate. But how accurate are these numbers?
A 2025 study published in Nature Scientific Reports compared three ring trackers (Oura, SleepOn, Circul) against polysomnography — the clinical gold standard that uses brain wave, eye movement, and muscle activity sensors. The results were sobering. For basic sleep-versus-wake detection, the Oura and SleepOn rings achieved about 85% accuracy — reasonable, and consistent with previous studies on healthy individuals. But for sleep stage classification (distinguishing wake, light sleep, deep sleep, and REM), the Oura ring managed only 53% accuracy, and the SleepOn ring 50%.
That is barely better than a coin flip for four categories. The sensitivity for individual stages ranged from 0.14 (REM sleep on the worst device) to 0.58 (light sleep on the best). And critically, the researchers found that "while some devices may demonstrate reasonable agreement with PSG on average, this agreement masks substantial individual-level inaccuracies." Your ring might say you got 90 minutes of deep sleep, but the actual number could be significantly different in either direction.
What the data is actually good for
This does not mean sleep trackers are useless. It means you need to read the data differently. Total sleep time at the group level was within 12 minutes of polysomnography for the Oura ring — close enough to be informative when tracked over weeks and months. The value of wearable data is in trends, not individual nights.
| Metric | Reliability | How to use it |
|---|---|---|
| Total sleep time | Good (within ~12 min at group level) | Track weekly averages, not individual nights |
| Sleep/wake detection | Moderate (~85% accuracy) | Useful for estimating sleep efficiency trends |
| Sleep stages (deep, REM, light) | Poor (~50-53% accuracy) | Treat as rough directional indicator only |
| HRV trends | Good for relative changes | Compare your own baseline over weeks, not absolute values |
| Resting heart rate | Good | Lower trends generally indicate better recovery |
HRV deserves special mention. While the Nature study focused on sleep staging, heart rate variability is arguably the most actionable metric for sleep optimization. Higher HRV generally indicates better autonomic nervous system balance and recovery. Rather than obsessing over whether you got 22 or 25 minutes of deep sleep (a distinction your tracker cannot reliably make), track your HRV trend over two to four weeks. If a protocol change consistently moves your HRV baseline up, that is a meaningful signal — even though the underlying sleep stage data may be fuzzy.
The orthosomnia trap
Researchers have identified a real clinical phenomenon where sleep tracking backfires. A 2023 paper in Nature and Science of Sleep by Jahrami et al. describes orthosomnia — "the obsessive pursuit of optimal sleep metrics based on fitness tracker or mobile phone app data." The paradox: people become so anxious about their sleep scores that the anxiety itself prevents them from sleeping. Dr. David Benavides, a sleep medicine specialist at Harvard Medical School, reports seeing an increasing number of patients with orthosomnia, bringing in wearable devices and worrying about their REM percentages — numbers their devices cannot even measure accurately.
A study of 75 sleep tracker users found that participants extended their time in bed specifically to improve their sleep scores and tried to eliminate any activity that might lower those scores. The researchers compare this anxiety to the documented phenomenon among diabetes patients using continuous glucose monitors, where constant data availability increases worry and psychological distress.
The practical guideline: check your sleep data once in the morning, note the trends over the week, then put the app away. If you find yourself checking before bed and feeling anxious about the upcoming night's numbers, that is a signal to take a break from tracking — possibly permanently.
How to Stack These Without Losing Your Mind
Knowing the research is one thing. Integrating five different optimization levers into a life that also involves work, family, and occasionally staying up late is another. The mistake most sleepmaxxers make is trying to implement everything simultaneously, creating an elaborate routine that becomes its own source of stress.
Start with the interventions that have the strongest evidence and require the least behavior change. Temperature is the easiest win: set your thermostat to 66°F tonight, and you are done. Light is the next priority: swap your evening living room bulbs to warm-white or tunable LEDs. These two changes require zero daily willpower once set up.
A sample evening-to-morning timeline: 2 hours before bed — warm shower/bath (10 min at 104-108°F). 1.5 hours before bed — dim lights, switch to warm/red lighting. 1 hour before bed — take magnesium glycinate + apigenin if using. 30 min before bed — screens off or orange-tinted if necessary. Morning — outdoor sunlight within first hour (5-20 min depending on conditions).
The supplement stack is optional and lower on the evidence hierarchy. If you want to try magnesium glycinate and apigenin, give it two to three weeks before evaluating. Track how you feel subjectively alongside any wearable data. If you notice nothing, stop. Experts warn that using supplements to compensate for persistent sleep trouble could mask a sleep disorder that needs professional attention.
Use your wearable to track HRV trends and total sleep time over weeks — not to grade individual nights. Add or change one variable at a time. If you start a warm bath routine and switch your lighting in the same week, you will not know which change made the difference.
| Priority | Intervention | Set-up effort | Daily effort | Evidence level |
|---|---|---|---|---|
| 1 | Bedroom temperature (65-68°F) | One thermostat adjustment | None | Strong (multiple reviews) |
| 2 | Evening warm lighting (2100-2700K) | Replace/program bulbs | None (automated) | Strong (Nature 2025) |
| 3 | Morning sunlight (5-20 min) | None | 5-20 minutes outside | Moderate (expert consensus) |
| 4 | Pre-bed warm bath (1-2h before) | None | 10-15 minutes | Strong (meta-analysis, 17 studies) |
| 5 | Mg glycinate + apigenin stack | Purchase supplements | 30 seconds | Weak-moderate (mouse synergy, no human combo trial) |
| 6 | Wearable trend tracking | Purchase device | 1 min morning check | Moderate (good for trends, poor for stages) |
Dr. Kashani's advice is worth ending on: "Your body wants to sleep and will sleep, as long as you don't let your mind get in the way." The irony of sleepmaxxing is that the people who need it least tend to pursue it most aggressively, while those with genuine sleep disorders often self-treat with TikTok hacks instead of seeing a doctor. If you have consistently practiced good sleep hygiene for several weeks and still struggle, skip the sleep stack and schedule a sleep study. The answer may be a medical condition, not a missing supplement.
Frequently Asked Questions
Is sleepmaxxing safe, or can optimizing sleep become unhealthy?
Most evidence-based sleepmaxxing strategies — controlling temperature, managing light exposure, maintaining a consistent schedule — are safe and recommended by sleep medicine physicians. The risk emerges when optimization becomes obsession. Researchers have documented a condition called orthosomnia, where people become so fixated on their sleep tracker data that the resulting anxiety worsens their sleep. If your sleep routine is causing you stress rather than reducing it, scale back. Dr. Shelgikar at the University of Michigan specifically warns that sleepmaxxing "can backfire if it turns what should be a restorative process into a high-pressure chore."
Should I take magnesium for sleep even if I'm not deficient?
The clinical evidence for magnesium as a standalone sleep aid in non-deficient people is weak. Dr. James Rowley at Rush University says there is "no good evidence that magnesium is a reliable sleep aid" for people with adequate levels. The more interesting research involves magnesium combined with apigenin, where a 2026 mouse study showed synergistic effects neither supplement achieved alone. However, no human clinical trial has tested this combination. If you have kidney disease or other conditions affecting magnesium metabolism, consult your doctor first — Dr. Shelgikar notes that some medical conditions can worsen with supplementation.
How accurate are Oura Ring and Apple Watch for tracking sleep stages?
A 2025 Nature Scientific Reports study comparing ring trackers against polysomnography found the Oura ring achieved about 85% accuracy for distinguishing sleep from wakefulness, but only 53% accuracy for classifying specific sleep stages (light, deep, REM). Total sleep time was within about 12 minutes of the gold standard at the group level. These devices are best used for tracking trends over weeks rather than analyzing individual nights. Only a lab-based sleep study can reliably determine your actual sleep architecture.
What is the single most effective sleepmaxxing strategy backed by research?
Temperature control has the broadest and most consistent evidence base. The warm bath meta-analysis (17 studies) shows reliable sleep onset improvements. Bedroom temperature between 65-68°F is supported by multiple expert recommendations and physiological research on thermoregulation. Unlike supplements or devices, temperature interventions require no ongoing purchases or daily habits — set the thermostat once and the benefit is continuous.
Do blue light blocking glasses actually work for sleep?
The most rigorous meta-analysis of randomized controlled trials (2025) found that blue light blocking glasses did not produce statistically significant improvements in objective sleep measures. However, the story is more nuanced than a simple yes or no. Most commercial glasses do not filter enough of the right wavelengths. Only brown-tinted lenses with high melanopic filtering showed meaningful melatonin protection in laboratory testing. A more effective strategy may be switching your home lighting to warm, tunable LEDs set below 2700K in the evening — this produced dramatically larger reductions in melatonin suppression than any glasses tested.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











