
The Estrogen Cliff That Reshapes Your Midsection
A woman who maintained the same weight through her 30s and early 40s steps on the scale at 52 and sees the same number. But her pants tell a different story. The waistband digs in where it never did before. This disconnect between total weight and body shape is the signature move of menopausal fat redistribution, and it has nothing to do with discipline or willpower.
The mechanism is hormonal and well-documented. During reproductive years, estradiol circulates at 100 to 250 pg/mL and actively directs fat storage toward the hips and thighs. Estrogen receptors in subcutaneous tissue respond to these signals by keeping fat deposited safely under the skin, away from organs. After menopause, estradiol plummets to around 10 pg/mL. The traffic signals go dark, and fat finds a new home.
That new home is visceral adipose tissue, the fat packed between and around abdominal organs. According to a review published in the journal Women's Health, visceral fat increases from 5 to 8 percent of total body fat in premenopausal women to 15 to 20 percent in postmenopausal women. The same review tracked VAT increasing at 8.2 percent per year before the final menstrual period and 5.8 percent per year after. Over a five-year window, postmenopausal women accumulated 49 percent greater intra-abdominal fat area than women who remained premenopausal.
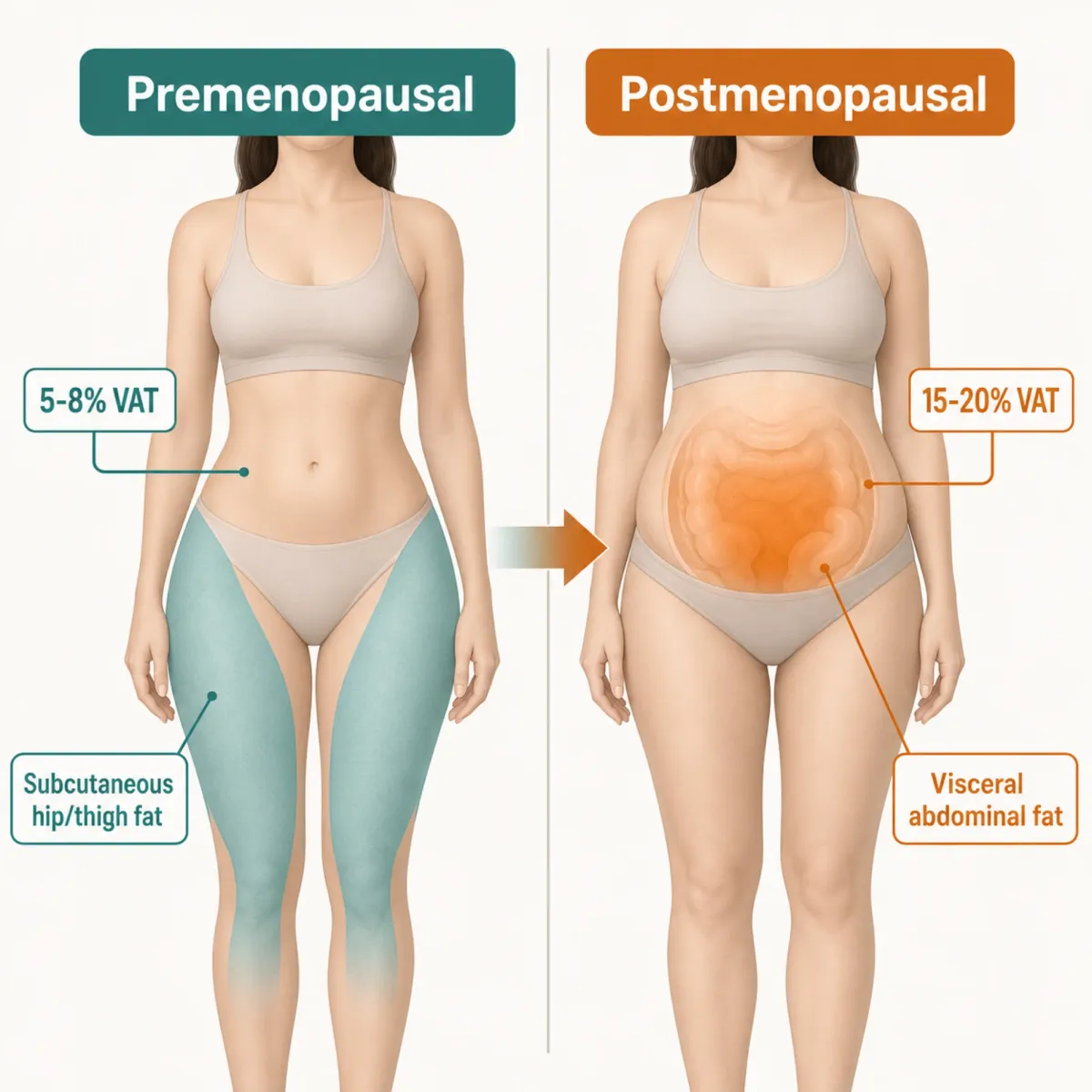
Think of estrogen as a parking attendant directing fat molecules into relatively harmless spots under the skin. When that attendant clocks out permanently, fat starts parking wherever there is space, and visceral compartments have plenty of it.
The metabolic engine slows down in parallel. JC Lovejoy's research at Pennington Biomedical Research Center followed 156 women over four years and found that fat oxidation declined 32 percent in women who went through menopause while remaining unchanged in premenopausal controls. Total daily energy expenditure dropped roughly 200 calories per day, with postmenopausal women showing a 9.3 percent reduction compared to 7 percent in those still cycling.
Lovejoy's team also discovered something counterintuitive: visceral fat began accumulating three to four years before menopause officially started, then plateaued afterward. The damage is largely done during the transition itself. By the time periods stop entirely, visceral fat has already found its footing.
Follicle-stimulating hormone plays its own role here. Research from the descriptive review in Clinical and Experimental Obstetrics & Gynecology points to work by Liu et al. (2017) showing that blocking FSH induces thermogenic adipose tissue and reduces body fat, suggesting the post-menopausal surge in FSH actively promotes visceral fat accumulation beyond what estrogen loss alone explains. It is a two-hit problem: estrogen drops and FSH rises, and both favor belly fat.
Tesamorelin: A Drug Built for One Problem, Borrowed for Another
Tesamorelin is a synthetic 44-amino-acid analogue of growth hormone-releasing hormone. The pituitary gland has receptors for GHRH. Tesamorelin binds them and stimulates natural growth hormone production, which in turn raises IGF-1 levels. Elevated GH and IGF-1 accelerate lipolysis, which is the breakdown of stored fat for energy.
The FDA approved tesamorelin under the brand name Egrifta in 2010 for a narrow indication: reduction of excess abdominal fat in adults with HIV-associated lipodystrophy. Antiretroviral therapy causes a distinctive pattern of fat accumulation around the midsection in many HIV patients, and tesamorelin was the first drug specifically approved to address it.
What caught the attention of menopause clinicians was not the HIV connection. It was the specificity. Unlike general weight loss drugs that reduce fat everywhere, tesamorelin showed a preference for visceral fat. In the pivotal JAMA trial led by Dr. Takara Stanley at Massachusetts General Hospital, subcutaneous fat did not change significantly (p=.29) while visceral fat dropped substantially. The drug seemed to know which fat to target.
Key distinction: Tesamorelin is not a weight loss drug. Most patients in clinical trials did not lose significant total body weight. What changed was where the fat was stored and how metabolically active it remained.
Off-label prescribing for menopausal belly fat has grown steadily. Clinics offering peptide therapy typically administer tesamorelin as subcutaneous injections five to seven days per week in multi-month cycles with programmed breaks. The standard dose mirrors the HIV-approved protocol: 2 mg daily via subcutaneous injection. The rationale is straightforward. Menopausal women experience visceral fat accumulation for hormonal reasons, and tesamorelin has demonstrated visceral fat reduction in controlled trials. Whether the mechanism translates identically across populations is the question that research has not fully answered.
What the Clinical Data Actually Shows
The strongest tesamorelin evidence comes from HIV populations, and the numbers are worth examining closely. Across two Phase III trials involving 806 HIV-infected patients with abdominal obesity, tesamorelin reduced visceral adipose tissue by approximately 15 percent over 26 weeks. The FDA defined clinical response as an 8 percent or greater VAT reduction. Sixty-nine percent of tesamorelin-treated subjects met that threshold compared to 33 percent receiving placebo.
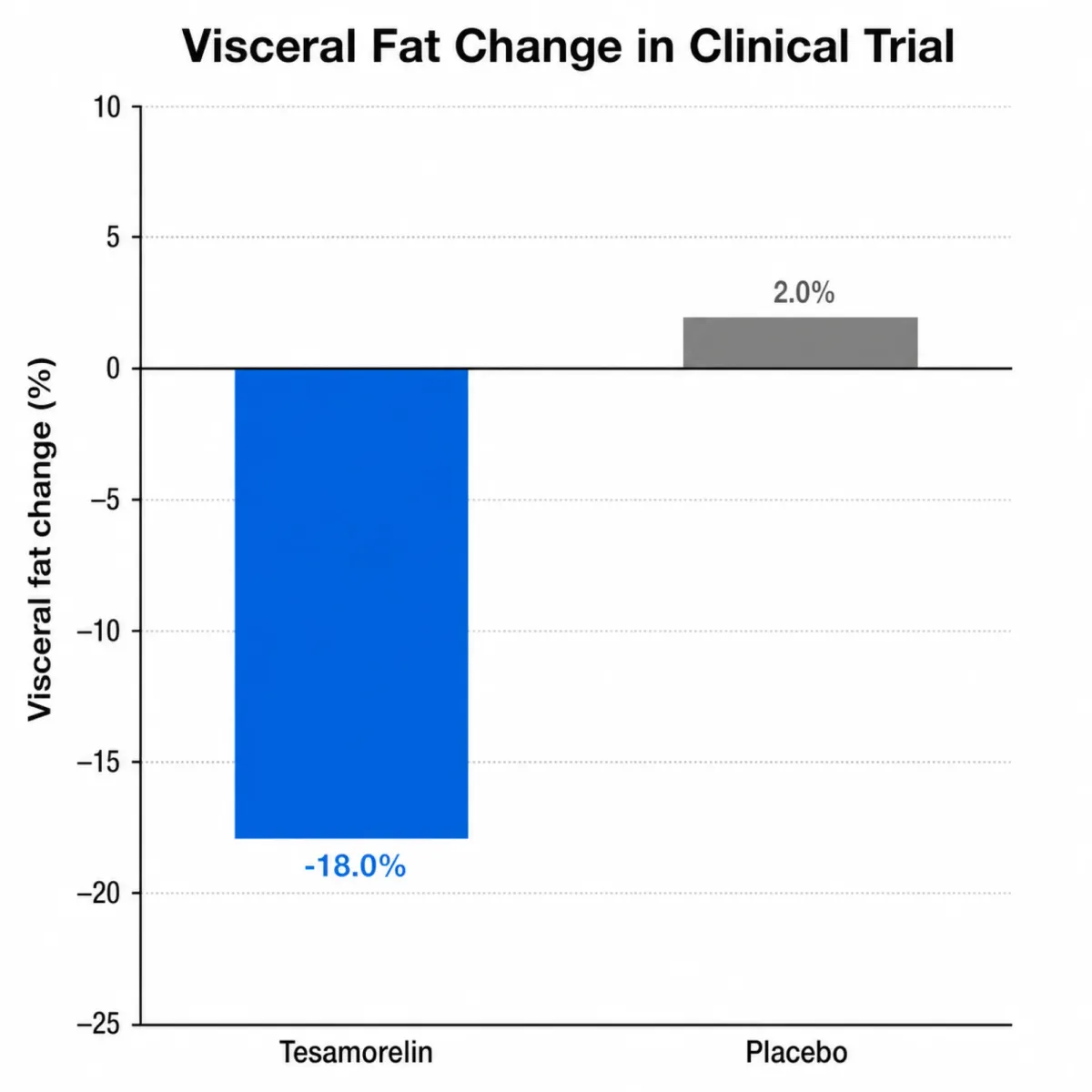
The smaller but more detailed JAMA trial from 2014 provides the granular data. Dr. Stanley's team randomized 50 patients and measured outcomes with CT imaging. Tesamorelin reduced VAT by a mean of 34 cm squared versus an 8 cm squared increase in the placebo group, a net treatment effect of 42 cm squared (p=.005). In percentage terms, that was a 9.9 percent decrease versus a 6.6 percent increase.
Beyond shrinking visceral fat, tesamorelin appears to improve the quality of remaining fat tissue. Research led by Jordan Lake at UT Health San Antonio, published with senior author Todd Brown from Johns Hopkins, analyzed the Phase III data and found that tesamorelin increased VAT density by 6.2 Hounsfield Units compared to 0.3 HU in the placebo group (p<0.0001). Higher tissue density in this context indicates less lipid content per unit of fat tissue. The fat that remained was metabolically healthier. Increases in adiponectin and IGF-1 correlated with these density improvements, and changes in fat density inversely correlated with total cholesterol and triglyceride changes.
The liver benefits added another dimension. Among the 806 Phase III patients, 64 percent had elevated liver enzymes at baseline. Those who achieved meaningful VAT reduction saw ALT decrease by 8.9 U/L, roughly 18 percent, while non-responders saw a 1.4 U/L increase. Thirty-five percent of responders achieved normal ALT levels versus 18 percent of non-responders.
| Outcome | Tesamorelin | Placebo | Significance |
|---|---|---|---|
| VAT reduction (JAMA trial) | -34 cm² | +8 cm² | p=.005 |
| VAT reduction (Phase III, 26 weeks) | ~15% | — | 69% achieved ≥8% reduction |
| Liver fat change | -2.0% | +0.9% | p=.003 |
| Subcutaneous fat | No significant change | No significant change | p=.29 |
| Fat density (VAT, HU) | +6.2 | +0.3 | p<.0001 |
A critical limitation: these trials enrolled HIV-positive patients, predominantly men (86 to 87 percent male), with a mean age around 48 to 50. The visceral fat in HIV lipodystrophy accumulates through drug-induced metabolic disruption, not estrogen loss. Whether the same magnitude of response occurs in postmenopausal women whose visceral fat has a completely different hormonal origin is genuinely unknown. A clinical trial registered on ClinicalTrials.gov (NCT06554717) is studying tesamorelin as an adjunct to exercise, which could generate non-HIV data, but results are not yet available.
Clinicians prescribing tesamorelin off-label for menopausal patients are extrapolating from HIV data and clinical observation. Some report visible reductions in waist circumference within three to six months. But anecdotal results from self-selected clinic patients who are also modifying diet, exercise, and sometimes taking HRT simultaneously do not carry the same weight as placebo-controlled trials.
The Other Peptides in the Conversation
Tesamorelin is not the only peptide being discussed in menopause-focused clinics. Two others appear frequently: AOD-9604 and the CJC-1295/Ipamorelin combination. Their evidence profiles look very different from tesamorelin's.
AOD-9604: The Fragment That Didn't Deliver
AOD-9604 is a modified fragment of human growth hormone, specifically amino acids 177 through 191. The theory was appealing: isolate the fat-burning portion of GH without the muscle-building or blood-sugar-raising effects. Early short-term studies generated excitement.
The excitement did not survive larger trials. A comprehensive meta-analysis covering over 900 participants across multiple human trials found no statistically significant difference in fat mass or body weight reduction between AOD-9604 and placebo. Confidence intervals crossed zero. The effect size was clinically negligible. The pharmaceutical company that developed it abandoned the program after Phase 2 trials failed to demonstrate efficacy.
AOD-9604 gained regulatory approval as a food ingredient in some jurisdictions but never as a pharmaceutical treatment. Despite this, it remains one of the most commonly offered peptides at cash-pay clinics marketing to menopausal women. The gap between its marketing presence and its evidence base is wide.
CJC-1295 and Ipamorelin: The Growth Hormone Stack
CJC-1295 is a synthetic peptide that extends the half-life of growth hormone-releasing hormone. Ipamorelin is a ghrelin mimetic that stimulates GH release without significantly affecting cortisol or prolactin. Combined, they are marketed as a sustained GH-boosting protocol for fat loss and body composition improvement.
The clinical evidence is thin. Human trials specifically examining fat loss from CJC-1295 and ipamorelin are limited or absent. No large randomized controlled trial has demonstrated meaningful fat reduction from this combination. Both peptides face regulatory restrictions as of April 2026, complicating their availability through legitimate compounding pharmacies.
| Peptide | Mechanism | Human Trial Evidence | FDA Status |
|---|---|---|---|
| Tesamorelin | GHRH analogue → GH/IGF-1 increase | Strong (800+ patients in Phase III) | Approved for HIV lipodystrophy |
| AOD-9604 | GH fragment (aa 177-191) | Failed (900+ patients, no effect vs placebo) | Not approved; food ingredient only |
| CJC-1295/Ipamorelin | Extended GHRH + ghrelin mimetic | Minimal (no large fat loss trials) | Not approved; regulatory restrictions |
| GLP-1 agonists | Appetite regulation, gastric slowing | Strong (thousands of patients) | Approved for weight management |
For context, the only category of peptide medications with strong clinical evidence for fat loss is GLP-1 receptor agonists like semaglutide and tirzepatide. Those drugs work through entirely different mechanisms (appetite regulation, gastric slowing) and produce total body weight loss rather than targeted visceral fat reduction. They are relevant to the menopausal belly fat conversation but are not peptides in the same growth-hormone-axis category as tesamorelin.
What Happens When You Combine HRT and Peptides
This is the question that menopausal women increasingly ask their clinicians, and the honest answer is that nobody has studied it properly.
What we know about HRT alone is encouraging. The OsteoLaus cohort study tracked 1,053 postmenopausal women aged 50 to 80 and found that current hormone therapy users had significantly lower visceral adipose tissue than never-users (P=0.02). Current users also showed lower BMI by 0.9 kg/m squared (P=0.03) and reduced android fat mass. Menopausal hormone therapy appeared to prevent the decade-long VAT gain that untreated women experienced.
Two findings from OsteoLaus temper the enthusiasm. First, past users showed no residual body composition advantages. Women who stopped HRT saw rapid rebound, losing whatever fat distribution benefits they had gained. The protection was present only while treatment continued. Second, HRT showed no benefit for lean body mass or muscle strength. It addressed fat distribution but not the muscle loss that also drives metabolic decline during menopause.
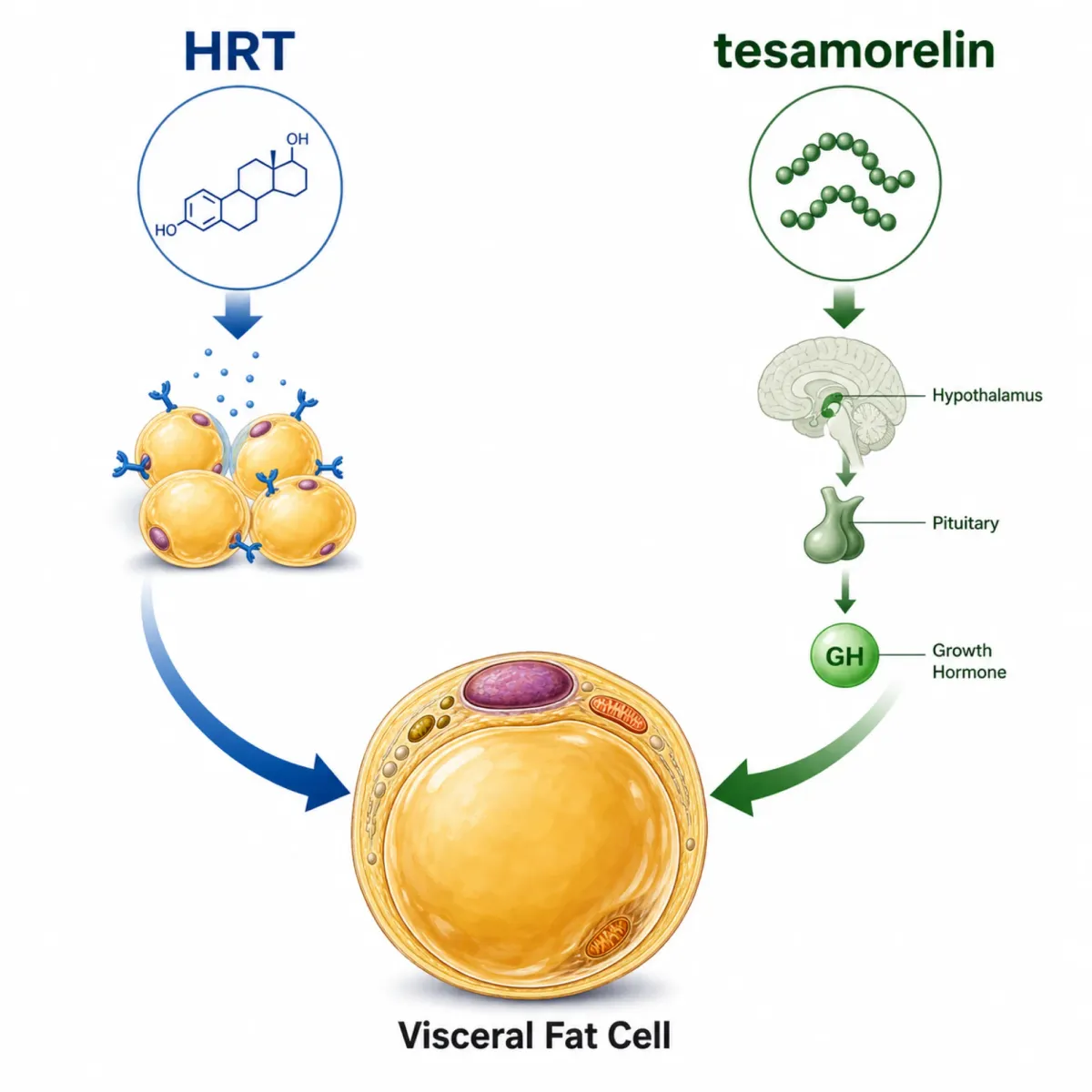
HRT restores estrogen signaling and redirects fat storage patterns, but it does not stimulate the growth hormone axis. Tesamorelin raises GH and IGF-1, promoting lipolysis specifically in visceral compartments. In theory, the two address different parts of the problem: HRT prevents new visceral fat accumulation by restoring the hormonal signal, while tesamorelin mobilizes existing visceral fat through the GH pathway.
Plausible, but unproven. No completed human randomized controlled trial has studied peptides specifically as HRT adjuncts in menopausal women. Clinicians who prescribe both are operating from mechanistic reasoning and patient-reported outcomes, not combination trial data. Baseline testing typically includes IGF-1, estradiol, FSH, LH, progesterone, hs-CRP, and metabolic panels before initiating any peptide alongside HRT.
For women already on HRT who still carry stubborn belly fat, the question is whether adding a peptide justifies the cost, daily injections, and extra monitoring. Without combination data, the answer sits squarely in the gray zone between biological plausibility and proof.
What Peptides Cannot Do and What They Cost
Tesamorelin is not a substitute for the foundational interventions that matter most during menopause. Sixty to 70 percent of middle-aged women gain weight during the menopausal transition, and the majority of that gain responds to resistance training, adequate protein intake, and sleep optimization before any injectable enters the picture.
Dr. Mary Claire Haver has noted that muscle mass declines 5 to 10 percent per decade after age 50, a trajectory that directly undermines metabolic rate. Resistance training two to three times weekly with progressive overload, combined with protein intake of 1 to 1.2 grams per kilogram per day, addresses this decline in ways that no peptide can replicate. Sixty-five percent of women aged 40 to 59 already have abdominal obesity, and the percentage climbs to nearly 74 percent after 60. These numbers reflect lifestyle and hormonal factors that peptides alone cannot reverse.
Women who do pursue tesamorelin should know what to expect. Meaningful results typically take three to six months. The drug reduces visceral fat specifically; it will not flatten a belly that carries significant subcutaneous fat. Total body weight may barely change. Women who step on the scale expecting dramatic drops will be disappointed even if their waist measurement improves.
Side effects in clinical trials included injection-site bruising (36 percent), paresthesia (21 percent), and arthralgia (14 percent). The JAMA trial documented a transient fasting glucose elevation at two weeks that normalized by six months, but HbA1c showed a modest increase of 0.20 percent in the tesamorelin group versus 0.02 percent with placebo. For women with existing insulin resistance, which is common during menopause, this warrants monitoring.
| Consideration | Detail |
|---|---|
| Timeline to results | 3-6 months for measurable visceral fat changes |
| Common side effects | Injection reactions, joint pain, numbness/tingling, fluid retention |
| Blood sugar impact | Transient glucose rise; HbA1c may increase slightly |
| What it targets | Visceral fat specifically; subcutaneous fat largely unchanged |
| What it does not do | Significant total weight loss, muscle building, skin tightening |
| Monitoring needed | IGF-1, fasting glucose, HbA1c, metabolic panels at regular intervals |
Cost is the unspoken barrier. Tesamorelin prescribed off-label is not covered by insurance for non-HIV patients. Monthly costs through compounding pharmacies or clinics typically run several hundred dollars, on top of the required blood work and physician monitoring. A six-month course with labs can easily exceed several thousand dollars out of pocket. For many women, this puts the drug out of practical reach regardless of its theoretical benefits.
Peptide marketing for menopausal belly fat has outpaced the evidence. Tesamorelin has real clinical data showing visceral fat reduction, though all of it comes from HIV populations. The off-label case rests on biological plausibility and clinical observation. AOD-9604 failed in trials. CJC-1295 and ipamorelin lack trials entirely. Any clinician presenting these peptides as proven solutions for menopausal belly fat is overstepping what the research supports.
Frequently Asked Questions
Is tesamorelin FDA-approved for menopausal belly fat?
No. Tesamorelin is FDA-approved only for excess abdominal fat in adults with HIV-associated lipodystrophy. Any use for menopausal belly fat is off-label, meaning a physician prescribes it based on clinical judgment rather than a specific FDA indication. There are no completed randomized controlled trials testing tesamorelin in menopausal women specifically.
How long does tesamorelin take to reduce belly fat?
Clinical trials showed measurable visceral fat reduction over 26 weeks of daily injections. Clinicians who prescribe it off-label for menopause report that some patients notice changes in bloating and energy within weeks, but measurable body composition changes typically take three to six months. Tesamorelin reduces visceral fat specifically, so the scale may not move significantly even when waist measurements improve.
Does AOD-9604 work for menopausal belly fat?
The evidence says no. A meta-analysis of over 900 participants found no statistically significant difference between AOD-9604 and placebo for fat mass or body weight reduction. The pharmaceutical company that originally developed it discontinued the program. Despite frequent marketing at peptide clinics, AOD-9604 has not demonstrated fat loss benefits in controlled human trials.
Can I take tesamorelin alongside HRT?
No completed human RCT has studied peptides as HRT adjuncts in menopausal women. Some clinicians prescribe both, reasoning that HRT addresses estrogen-related fat redistribution while tesamorelin targets the GH axis. This combination requires careful monitoring of metabolic markers, IGF-1 levels, and blood sugar. Discuss the potential benefits and risks with a physician experienced in both therapies before combining them.
Why does belly fat increase during menopause even without weight gain?
Estrogen decline shifts fat storage from subcutaneous depots in the hips and thighs to visceral compartments around abdominal organs. This redistribution begins three to four years before menopause and occurs even in women whose total body weight remains stable. Additionally, rising FSH levels after menopause independently promote visceral fat accumulation, creating a dual hormonal driver.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











