
Why Peptide Breaks Are Discussed at All
Peptide cycling sounds precise online: run this for a few weeks, stop for a few weeks, repeat. The evidence is messier. A break can mean a planned pause in an approved medication, a lab-guided reassessment of an endocrine therapy, the end of a short-term recovery experiment, or an urgent stop because a product source or side effect looks unsafe.
"Peptides" is not a single medical category. Dr. Cate Varney at UVA Health describes the market as stretching from FDA-approved GLP-1 receptor agonists to unregulated compounds with minimal or no human safety data. The same word can refer to semaglutide prescribed for obesity, tesamorelin prescribed for HIV-associated lipodystrophy, a topical copper peptide in skin care, or a gray-market vial labeled BPC-157.
For YMYL health decisions, "cycle peptides" should usually mean "build a reason to pause and reassess," not "copy a calendar from a forum."
The practical reason breaks are discussed is simple: living systems adapt. Think of a receptor like a doorbell. If someone presses it once, the house responds. If someone leans on it all day, the household starts ignoring the sound, disconnecting the chime, or changing how the signal is handled. In pharmacology, that rough idea shows up as desensitization, tachyphylaxis, tolerance, and receptor downregulation.
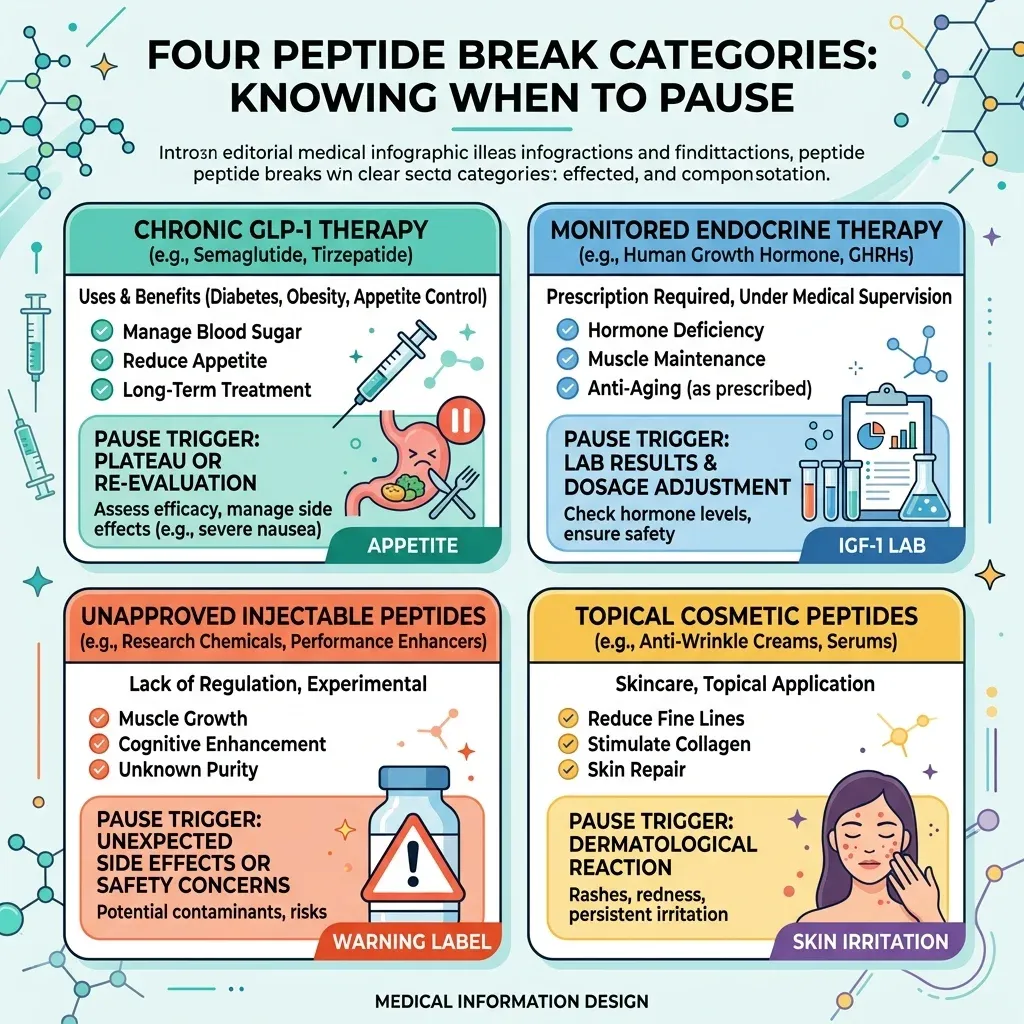
| Peptide situation | What a break usually means | Why it should not be guessed |
|---|---|---|
| Approved chronic therapy, such as a GLP-1 drug | A supervised discontinuation or change in treatment | Stopping can reverse benefits and needs follow-up planning |
| Approved endocrine therapy, such as tesamorelin | A lab-guided pause, discontinuation, or risk review | Labeling ties stop decisions to IGF-1, glucose, malignancy, and adverse reactions |
| Unapproved injectable or compounded peptide | A safety stop until a clinician reviews product, route, and symptoms | FDA and medical experts describe unknown safety profiles and product-quality risks |
| Cosmetic topical peptide | Usually a skin-tolerance or irritation pause | Topical exposure is different from systemic injection |
A better question than "What cycle does the internet use?" is: what biological system is being pushed, what objective marker can show stress or loss of benefit, and what would make a clinician stop?
This also helps separate two ideas that often get blurred together. One is pharmacology: receptors, hormones, glucose, appetite, immune response, or tissue repair signals may change with exposure. The other is product quality: an unapproved vial may be mislabeled, contaminated, or used by a route with little safety information. A break can address the first problem only if the product and diagnosis are sound. It cannot make a questionable product clean.
Desensitization Is Real, but It Does Not Apply to Every Peptide
Desensitization is not wellness slang. ScienceDirect defines receptor downregulation as prolonged receptor stimulation leading to degradation after desensitization and reversible endocytosis. The same source explains that receptor concentration and affinity can decrease after ligand binding and activation, and that changes in receptor number can help explain tolerance, tachyphylaxis, and desensitization.
That does not prove that every peptide supplement needs a neat on/off cycle. It proves a narrower point: if a compound repeatedly pushes a receptor system, adaptation is a real possibility. Growth hormone secretagogues are a good example because they act on hypothalamic and pituitary pathways. ScienceDirect describes growth hormone secretagogues as agents that stimulate growth hormone release through specific receptors in the hypothalamus and pituitary.
That system is more like a thermostat than a light switch. If you keep forcing heat into the room, the thermostat, furnace, and vents all become part of the response. Growth hormone secretagogues can influence growth hormone and, in some settings, ACTH, cortisol, and prolactin, which is why judging them by "I feel better" is too crude.
| Claim type | Evidence strength | Safer takeaway |
|---|---|---|
| Receptors can desensitize after repeated stimulation | Supported by pharmacology references | Use as a general mechanism, not a personal schedule |
| Every peptide needs the same fixed break | Not supported as a universal rule | Separate systemic injections, approved drugs, and topical products |
| Popular cycle calendars are medically proven | Often weak or protocol-based | Ask what lab, symptom, or endpoint justifies the pause |
If benefit fades, dose escalation is not the only move. A plateau can be a reason to reassess the original goal, product source, route, adverse effects, and objective markers before continuing.
That is why this guide avoids giving exact cycles for CJC-1295, ipamorelin, BPC-157, TB-500, or similar gray-market peptides. The fetched sources contained plenty of specific schedules, but most came from clinics, vendors, PDFs, or user discussions rather than high-quality trials designed to answer "how long should a person use this, then stop?" For a health article, the honest answer is less convenient: the break should follow the mechanism, the evidence level, and the monitoring plan.
GLP-1 Breaks Are Not Detoxes
GLP-1 receptor agonists are where casual cycle talk can become especially misleading. These drugs are often prescribed as ongoing treatment for obesity or diabetes, not as a hobby cycle. Stopping may be appropriate for side effects, pregnancy planning, access problems, surgery guidance, or a clinician's risk-benefit decision, but it should not be framed as a detox.
A Cambridge team led by Brajan Budini and Steven Luo reviewed and modeled GLP-1R discontinuation data. The university report says the team examined 48 relevant studies, including 36 randomized controlled trials and 12 non-randomized studies. From the trials with longer follow-up, they modeled what happened after people stopped.
The headline was blunt: by 52 weeks after discontinuation, people had regained 60% of their original weight loss. The same report projected that regain begins to plateau around 60 weeks, with about 25% of initial weight loss potentially sustained long term.
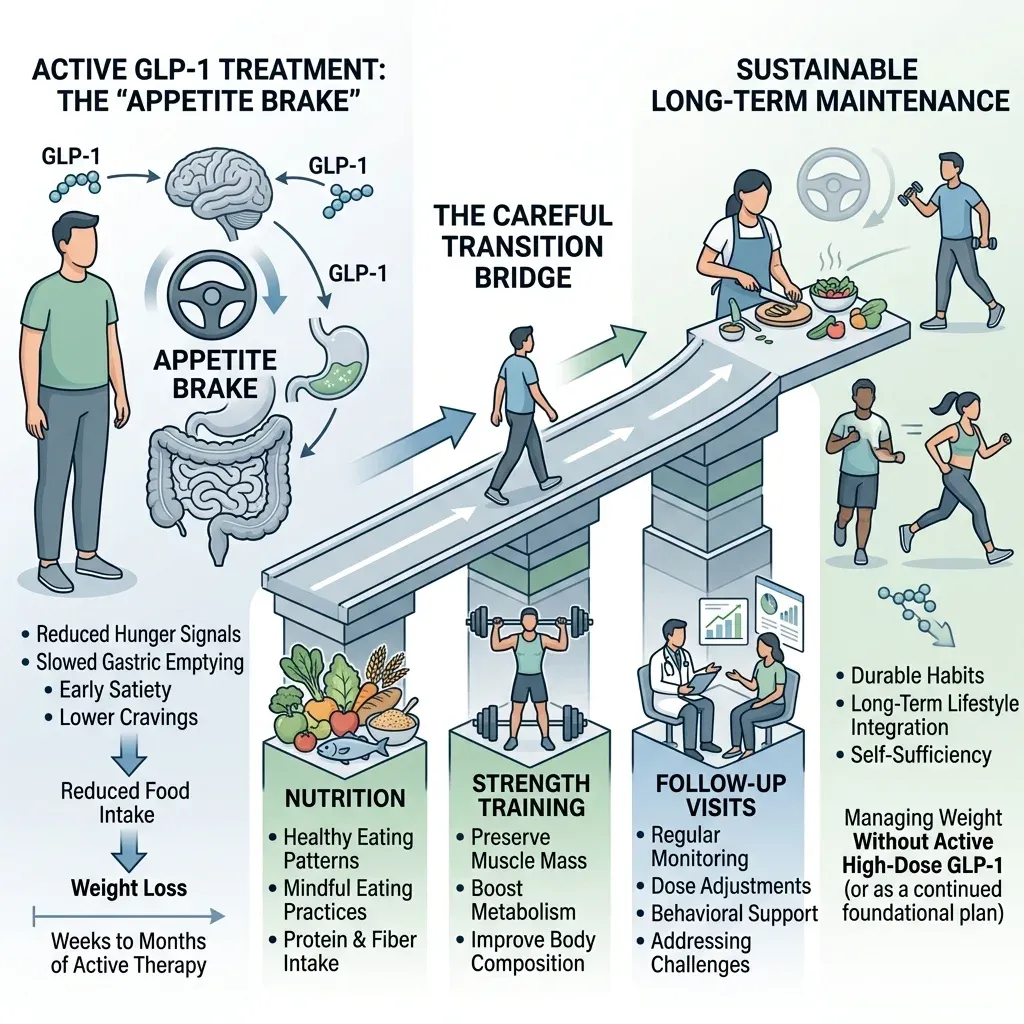
Budini's brake analogy is useful: GLP-1 drugs press down appetite signals. When the drug stops, the foot comes off the brake. That does not mean failure. It means the break has to be planned like a bridge, with nutrition, resistance training, follow-up, and expectations, because appetite biology is no longer being pharmacologically assisted.
There is another unresolved issue. Cambridge noted that studies suggest 40% to 60% of weight lost during treatment can be lean mass, and Budini warned that researchers do not yet know whether regained weight restores muscle, fat, or both. "Just take a break" is too casual for this class.
A GLP-1 pause should be a medical transition plan, not a receptor-cleanse ritual. If someone stops, the conversation should move quickly to appetite rebound, blood sugar if relevant, nutrition adequacy, muscle preservation, and follow-up timing.
Weight regain after stopping does not prove the medication was "bad" or that the body became lazy. GLP-1 drugs change appetite signaling while they are being used. A pause is closer to removing scaffolding from a building under repair: the structure may stand better if the support work is finished, but you do not yank the scaffolding away and hope.
Growth Hormone Secretagogues Need Monitoring, Not Guesswork
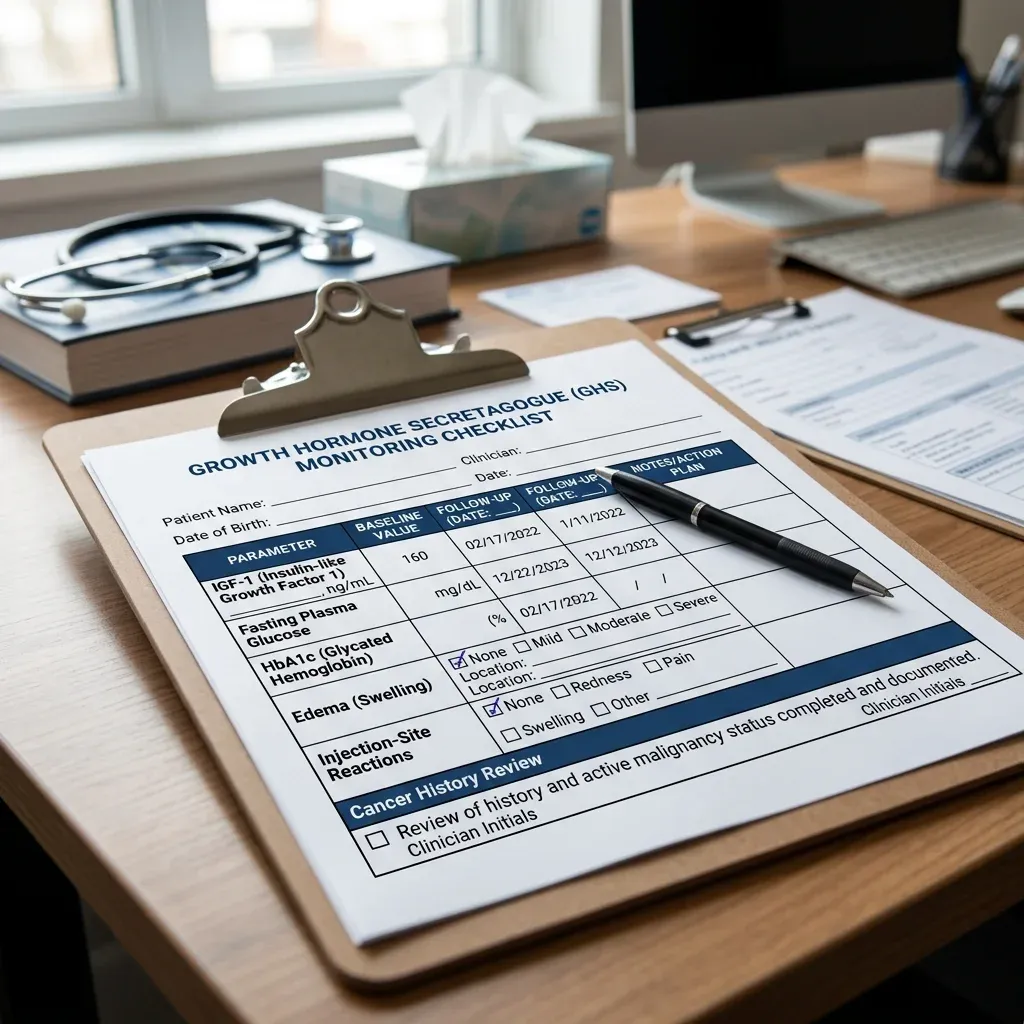
Growth hormone secretagogues are where break decisions should move from vibes to labs. Tesamorelin is the clearest example because it has FDA labeling. The EGRIFTA SV label says tesamorelin stimulates growth hormone production and increases serum IGF-1. NCBI LiverTox similarly describes tesamorelin as a growth hormone-releasing hormone analogue that increases growth hormone and stimulates hepatic IGF-1 production.
The label does not say, "cycle it whenever you feel like it." It says the effects of prolonged IGF-1 elevations are unknown, recommends IGF-1 monitoring, and says clinicians should consider discontinuing EGRIFTA SV in patients with persistent IGF-1 elevations. In older EGRIFTA trial data, 47% of treated patients had IGF-1 levels greater than 2 standard deviation scores after 26 weeks, and 36% had levels greater than 3 standard deviation scores.
That is the difference between evidence-based pausing and internet cycling. A lab is a dashboard. If the oil light comes on, you do not solve the problem by driving in a more confident mood. You stop, inspect, and decide whether the trip should continue.
The same label includes other stop-and-review points. EGRIFTA SV is contraindicated in active malignancy, and the label says to discontinue if there is evidence of recurrent malignancy. It also warns about fluid retention, glucose intolerance or diabetes, hypersensitivity, injection-site reactions, and increased mortality concerns in acute critical illness.
For glucose, the label reports that by Week 26, elevated HbA1c of at least 6.5% occurred in 5% of EGRIFTA-treated patients and 1% of placebo patients, with a hazard odds ratio of 3.3. That does not mean every person will have a glucose problem. It means glucose belongs on the monitoring list.
With growth hormone-related peptides, "when to take a break" is often when the monitoring plan says the risk-benefit balance has changed. Persistent IGF-1 elevation, worsening glucose, fluid retention, suspected hypersensitivity, or cancer-history concerns are not optimization details. They are reasons to pause and contact the prescribing clinician.
This is where "cycle" becomes the wrong word. A cycle implies a repeatable routine. Monitoring implies judgment. If a lab is abnormal, if edema or carpal-tunnel-like symptoms appear, or if glucose control worsens, the decision is not to wait out a rest period and restart. It is to ask whether the original indication still justifies the risk.
Cosmetic and Research Peptides Change the Risk Calculus
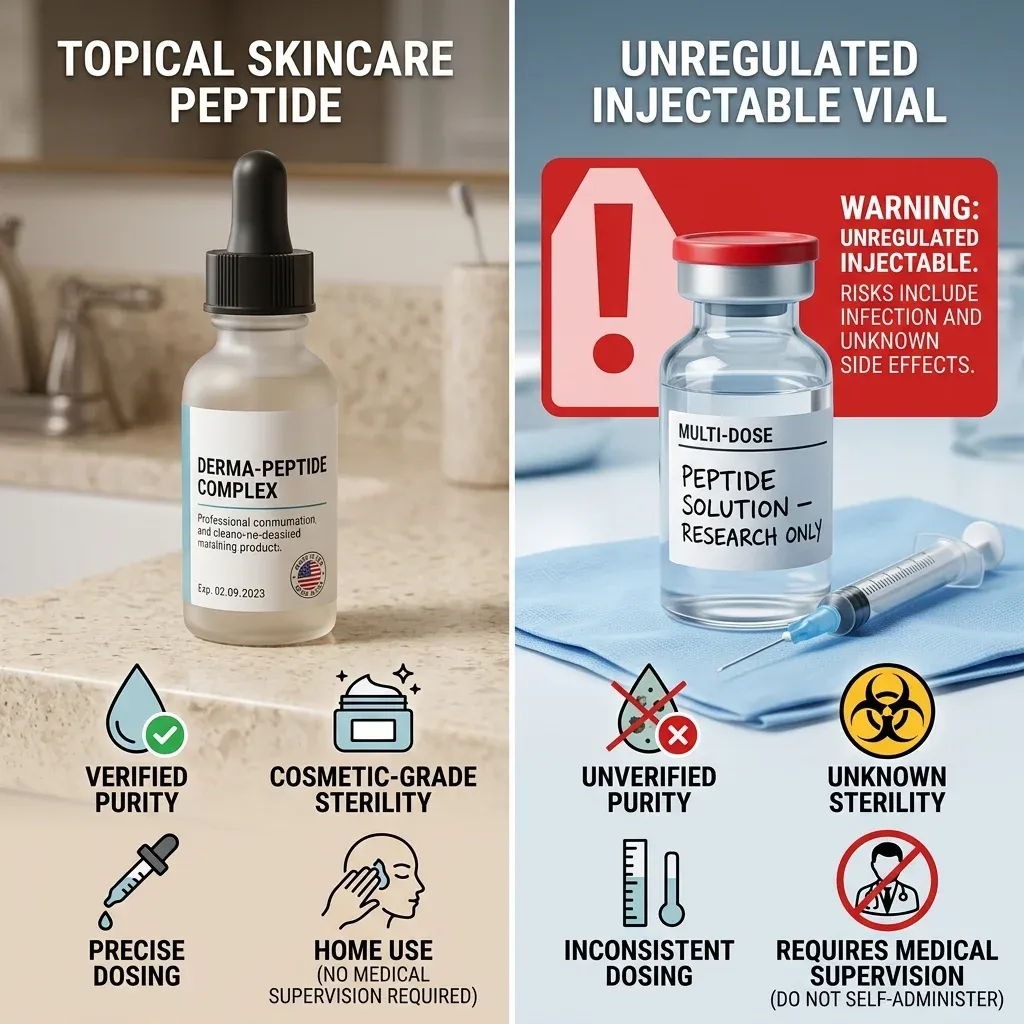
A topical cosmetic peptide and an injected research peptide do not deserve the same risk conversation. A face serum that irritates your skin may call for a product pause and a dermatology review. A self-injected unapproved peptide raises questions about sterility, dose, route, identity, contamination, and whether anyone is monitoring the organ system being pushed.
Dr. Varney makes that split clear. She told UVA Today that for injury-recovery peptides such as BPC-157 and TB-500, animal studies show promise, but human clinical evidence is essentially nonexistent. She also warned that non-FDA-approved peptides have largely unknown side-effect profiles because of the lack of human trials.
Her product-quality concerns are not abstract. UVA's report cites contamination with toxic elements such as arsenic and lead, variable purity, dosing errors, counterfeit products, and serious complications such as compartment syndrome. It also notes that one analysis found nearly one-quarter of tested products contained undisclosed compounds.
The FDA's compounding risk page gives more reason to slow down. FDA lists potential significant safety risks for several peptide bulk substances, including GHRP-2, GHRP-6, ibutamoren, ipamorelin, and kisspeptin-10. For GHRP-6, FDA describes immunogenicity concerns and possible effects on cortisol and blood glucose. For ipamorelin acetate, FDA says it lacks sufficient information to know whether certain injectable routes would harm humans.
Cosmetic tanning peptides deserve their own warning. Dr. Varney said melanotan peptides can induce skin darkening, but unregulated products are not FDA-approved for tanning and have safety concerns, including case reports of melanomas emerging from existing moles shortly after melanotan use.
With unapproved injectables, the safest break may be a full stop until a clinician reviews the product, symptoms, route, and reason for use. The risk is bigger than "losing sensitivity." The vial itself may be the problem.
Topical cosmetic peptides sit at the other end of the spectrum. They may still irritate skin or interact badly with a routine, but they do not create the same systemic uncertainty as injecting a research peptide into muscle or subcutaneous tissue. If a skin product stings, burns, triggers a rash, or worsens a condition, pause it and simplify the routine. If an injection causes swelling, severe pain, fever, spreading redness, numbness, or pressure, that is no longer a cosmetic troubleshooting problem.
When to Pause, Reassess, or Stop
A break is most defensible when it answers a specific clinical question. Has the target improved? Has the benefit plateaued? Are labs moving in the wrong direction? Did a side effect appear? Is the product source uncertain? Those are different questions, and they do not all lead to the same answer.
| Trigger | Why it matters | Likely next step |
|---|---|---|
| Persistent IGF-1 elevation during tesamorelin therapy | FDA labeling says prolonged IGF-1 elevation has unknown effects | Pause or discontinue only with the prescribing clinician |
| Rising glucose or new diabetes concern | EGRIFTA SV labeling warns about glucose intolerance and diabetes | Check glucose status and reassess benefit |
| Evidence of recurrent malignancy | EGRIFTA SV labeling says to discontinue if recurrence appears | Stop and obtain medical review |
| Unapproved peptide, unclear source, or injection complication | FDA and UVA describe contamination, dosing, and unknown-safety risks | Stop use and seek medical care |
| Planned GLP-1 discontinuation | Cambridge data show substantial weight regain after stopping | Build a transition plan for appetite, nutrition, training, and follow-up |
There is also a softer pause trigger: no measurable benefit. If a peptide was started for a defined goal, and the goal has not moved, the next step is not automatically a longer run. It may be confirming the diagnosis, checking whether the product is legitimate, changing the treatment plan, or stopping.
Write down the stop rules before starting. A reasonable plan names the goal, the marker being followed, the side effects that end the trial, and the clinician who owns the decision.
A written stop rule also protects against the sunk-cost trap. People are more likely to continue a risky or useless intervention after paying for vials, consults, or subscriptions. The better plan is decided before the first dose: what outcome would count as success, what finding would count as harm, and what date or lab result forces a reassessment instead of another refill.
A Safer Framework Than Online Cycles
The safer framework is boring, which is why it works. Start by naming the peptide class. Then ask whether the product is approved, compounded, cosmetic, or research-grade. Then identify what system it affects. Finally, decide what objective signal would justify continuing, pausing, or stopping.
That framework avoids two common mistakes. The first is treating all peptides as receptor-fatigue problems. The second is treating all breaks as harmless. GLP-1 discontinuation can mean appetite rebound. Tesamorelin continuation can mean lab monitoring. Unapproved injectables can mean product-quality danger. Topical cosmetic peptides can mean local irritation rather than systemic endocrine risk.
For readers, the most useful "exactly when" is not a private dosing calendar. It is a list of moments that should trigger a pause: abnormal labs, new or worsening symptoms, suspected contamination, unclear dosing, loss of meaningful benefit, pregnancy or pregnancy planning, cancer-history concerns, infection signs at an injection site, or a plan to stop a chronic drug without follow-up support.
That is less exciting than a perfect cycle chart. It is also much closer to the evidence.
Frequently Asked Questions
Should everyone cycle peptides?
No. "Peptides" includes approved drugs, endocrine therapies, topical cosmetic ingredients, and unapproved injectables. The reason to pause depends on the peptide, goal, product quality, side effects, and monitoring plan.
Are online peptide cycle calendars evidence-based?
Some calendars reflect clinic protocols or user communities, but many popular schedules are not proven by rigorous trials of optimal break timing. Use them as a reason to ask better questions, not as personal medical instructions.
Is stopping GLP-1 medication the same as taking a peptide break?
No. GLP-1 discontinuation can lead to appetite rebound and weight regain. Cambridge researchers reported substantial regain after stopping, so any pause should be planned with the prescribing clinician.
What peptide side effects mean I should stop and call a clinician?
Seek medical advice for allergic symptoms, severe injection-site reactions, signs of infection, fluid retention, glucose changes, pregnancy concerns, cancer-history concerns, or any side effect from an unapproved or uncertain product source.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











