
Why Peptide-Cancer Headlines Get Ahead of the Evidence
A peptide headline can sound more certain than the science behind it. One article may warn that a compound "feeds cancer." Another may suggest a drug class lowers cancer risk. Both can be partly true, partly incomplete, and easy to misread if the word "peptide" is treated as one category.
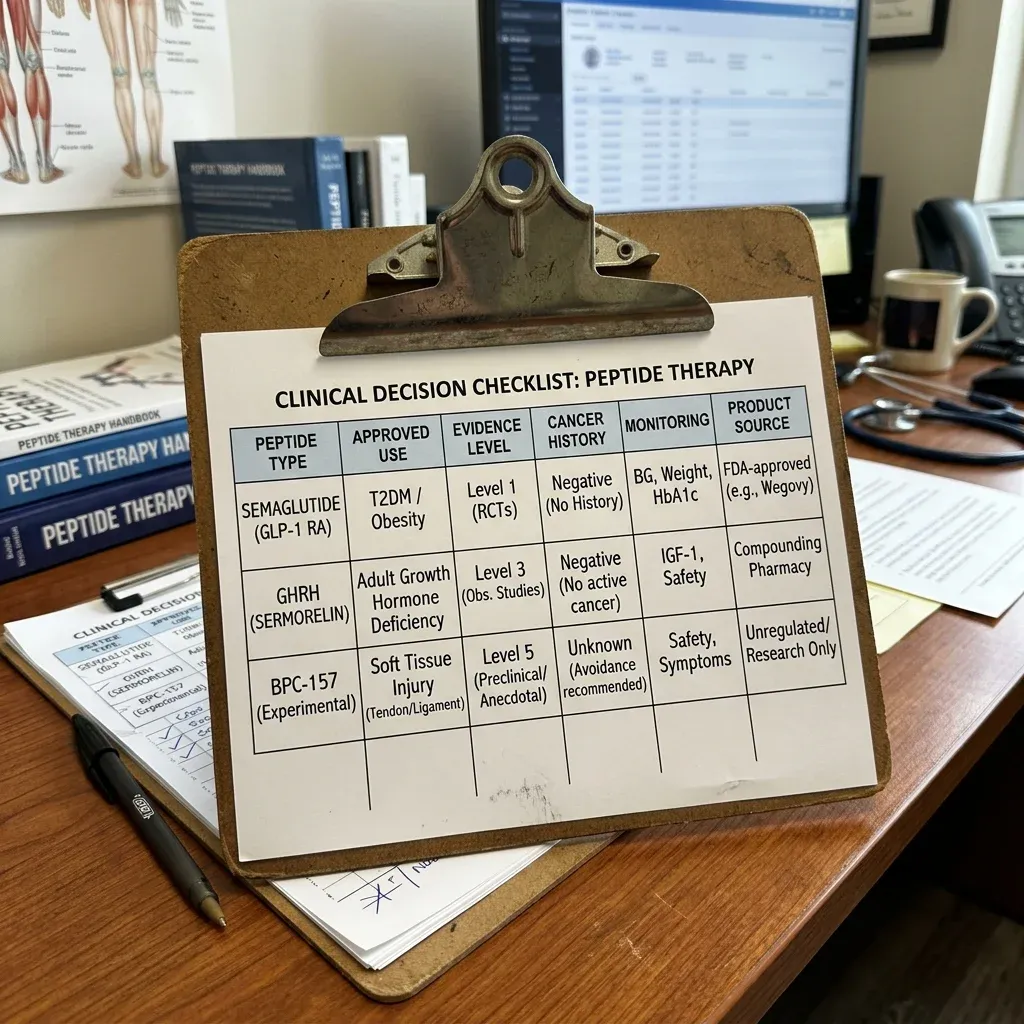
The first split is simple: approved medicines are not the same as wellness or research peptides. Dr. Cate Varney, director of obesity medicine at UVA Health, describes peptides as a broad group ranging from FDA-approved GLP-1 medicines to unregulated compounds sold for anti-aging, tanning, and injury recovery, many with minimal or no human safety data according to UVA Today.
Think of "peptide" like "vehicle." A crash-tested ambulance, a racing motorcycle, and a homemade cart all move on wheels, but they do not have the same safety record. In the same way, semaglutide, tesamorelin, melanotan, BPC-157, TB-500, CJC-1295, and ipamorelin should not be judged by one headline.
The cancer question also changes depending on the kind of evidence. A randomized trial can test whether people assigned to a medicine had more cancer events than people assigned to a comparator. A case report can warn that something suspicious happened in one patient. An animal study can show a mechanism that deserves caution. None of those can automatically replace the others.
The practical rule: ask what kind of peptide, what kind of evidence, what kind of cancer signal, and whether the product is an approved monitored medicine or an unregulated compound.
The FDA has placed several compounded peptide bulk substances on risk lists because of concerns such as immunogenicity, peptide-related impurities, limited safety information, and route-specific uncertainty in its compounding safety table. That is not the same as saying each peptide causes cancer. It means the evidence is not strong enough to treat them as casually interchangeable with approved drugs.
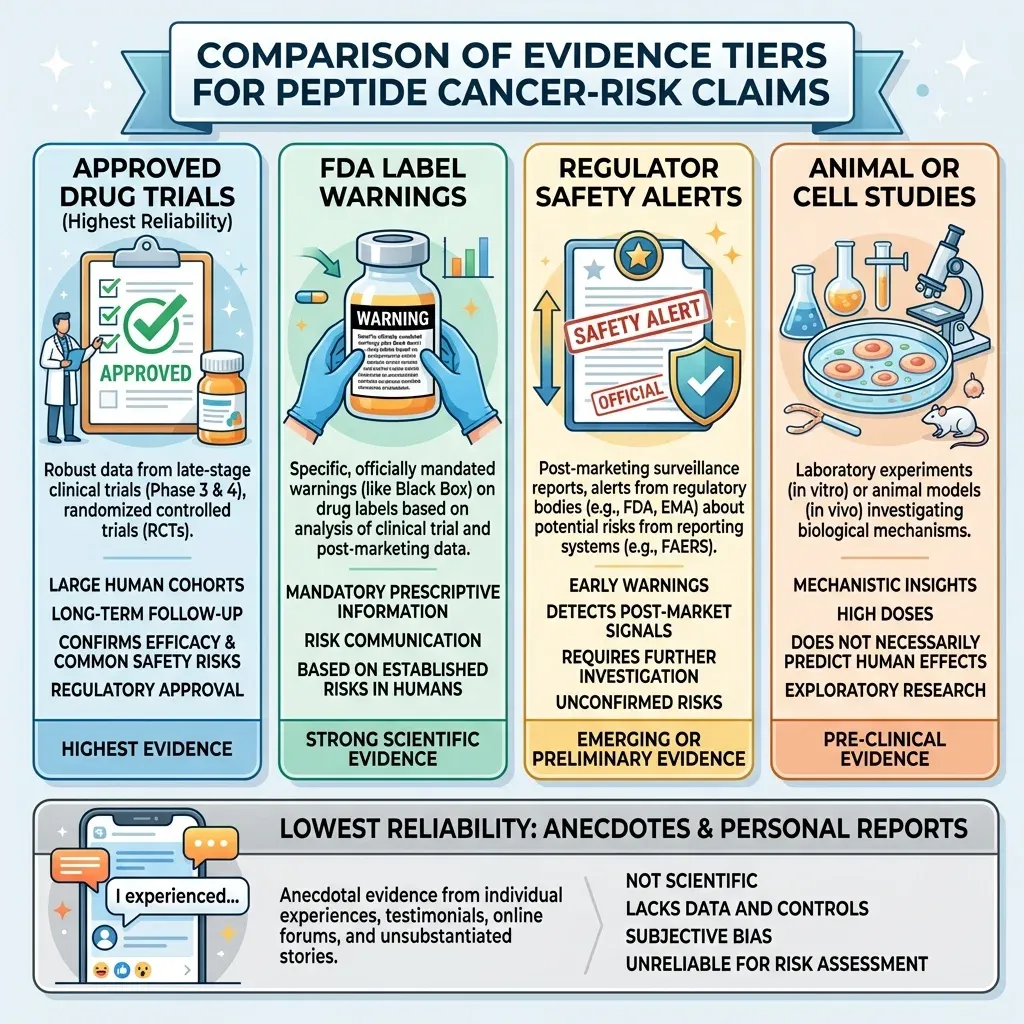
| Evidence type | What it can say | What it cannot prove alone |
|---|---|---|
| Randomized trials and meta-analyses | Whether cancer events were higher or lower in studied groups | Long-latency risk if follow-up is short |
| FDA labels and regulator warnings | Known contraindications, monitoring needs, and safety uncertainties | That every related wellness peptide has the same risk |
| Animal, cell, and mechanism studies | Why a pathway might matter biologically | Human cancer causation |
| Case reports | Signals that deserve attention | Population-level risk or causality |
For readers, the useful move is not panic or reassurance. It is sorting. The next sections separate the better-studied GLP-1 category from growth-hormone-axis peptides, tanning peptides, and regenerative peptides that are often marketed far beyond their evidence.
Approved GLP-1 Medicines Have the Most Human Data
GLP-1 receptor agonists get pulled into peptide-cancer headlines because they are peptide-like medicines and because early thyroid concerns came from biology that looked worrying in animals. The human data are much more nuanced.
Gianluca A. Silverii and colleagues pooled 50 randomized controlled trials lasting at least 52 weeks and found no significant difference in overall cancer risk for GLP-1 receptor agonists compared with controls, with an MH-OR of 1.05 and a 95% confidence interval of 0.98 to 1.13. That does not mean "zero risk." It means the pooled trial data did not show a clear overall cancer increase.
The same meta-analysis did find a thyroid cancer signal, with an MH-OR of 1.55 and a 95% confidence interval of 1.05 to 2.27. The authors did not present that as settled causation. They described it as a signal needing further study, which matters because rare thyroid outcomes are hard to pin down when trial cancer events are few.
Another systematic review focused on gastrointestinal cancers and included 90 randomized controlled trials with 124,791 participants. It reported no significant association with any gastrointestinal cancer, with an RR of 0.99 and a 95% confidence interval of 0.86 to 1.13. Average follow-up was 3.1 years per participant, which is helpful but still short for some slow-growing tumors.
The picture gets more interesting when studies look at cancers linked to obesity. A meta-analysis of 24 studies involving 3,960,974 patients found GLP-1RA use associated with lower obesity-related cancer risk within ten years, with an RR of 0.70 and a 95% confidence interval of 0.54 to 0.89. The authors still called for more work to establish causality, which is the sober way to read it.
So the GLP-1 answer is neither "these drugs cause cancer" nor "these drugs prevent cancer." It is: the best human evidence so far is relatively reassuring for overall and gastrointestinal cancer risk, thyroid signals remain under study, and long-term cancer-specific follow-up still matters.
Growth-Hormone Axis Peptides Raise a Different Question
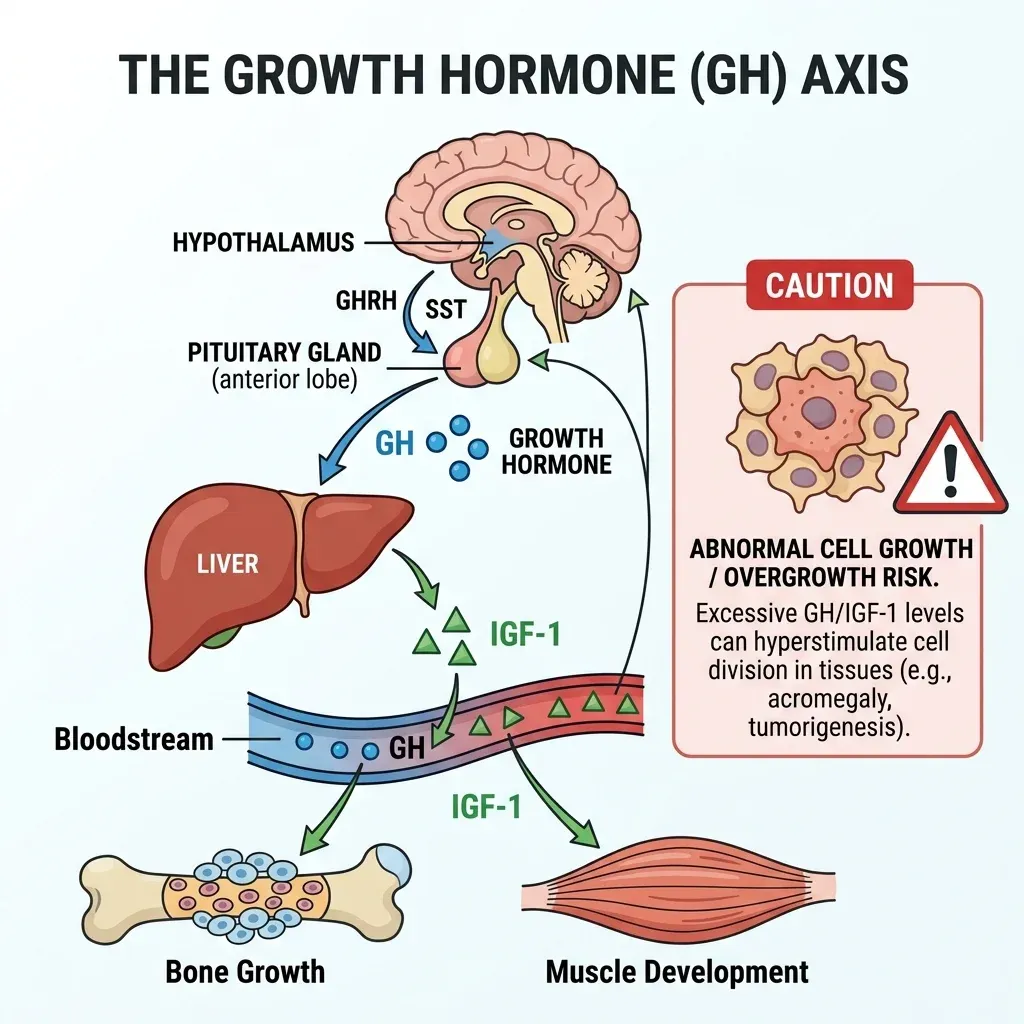
Growth-hormone-axis peptides are a different conversation because they are built around growth signaling. Tesamorelin is the best example because it is an FDA-approved growth hormone-releasing factor analog for reducing excess abdominal fat in HIV-infected adults with lipodystrophy according to the EGRIFTA WR label.
Here the FDA label is direct. EGRIFTA WR is contraindicated in patients with active malignancy under the contraindications section. The label says a preexisting malignancy should be inactive and treatment complete before starting therapy, and that clinicians should discontinue the drug if there is evidence of recurrent malignancy under warnings and precautions.
The mechanism explains the caution. The label states that EGRIFTA WR stimulates GH production and increases serum IGF-1, a growth factor, and that the effects of prolonged IGF-1 elevations are unknown in section 5.2. Think of IGF-1 as a construction permit. In the right tissue, at the right dose, under supervision, construction can be useful. In or near a cancer-prone site, the same growth permission is why clinicians slow down.
The monitoring numbers are not subtle. Among patients who received EGRIFTA for 26 weeks, 47% had IGF-1 levels greater than 2 SDS and 36% had SDS greater than 3. The label advises monitoring IGF-1 and considering discontinuation when elevations persist in patients with persistent elevations.
| Peptide category | What the evidence supports | Cancer-risk interpretation |
|---|---|---|
| Tesamorelin | Approved for HIV-associated lipodystrophy, with label monitoring | Clear malignancy precautions and IGF-1 monitoring |
| Ipamorelin | Compounding safety concerns listed by FDA | Insufficient safety information for certain injectable routes |
| CJC-1295 | Limited clinical data in FDA compounding review | Safety uncertainty, not proven human cancer causation |
That distinction matters for CJC-1295 and ipamorelin. The FDA says compounded ipamorelin acetate may pose immunogenicity risk and that the agency lacks sufficient information to know whether certain injectable routes would cause harm in humans in its Category 2 table. For CJC-1295, the FDA notes limited clinical data and serious adverse events including increased heart rate and systemic vasodilatory reaction in the withdrawn nominations table.
The practical takeaway is not that every GH-axis peptide causes cancer. It is that a growth-signal peptide used outside a clear indication, without cancer history review, IGF-1 monitoring, product-quality assurance, and follow-up, is asking users to carry uncertainty that should belong in clinical supervision.
Melanotan and Tanning Peptides Are the Clearest Red-Flag Category
Melanotan is where the cancer conversation becomes less abstract. It is not a general "cell growth" worry. It directly targets pigment biology, and regulators have been blunt.
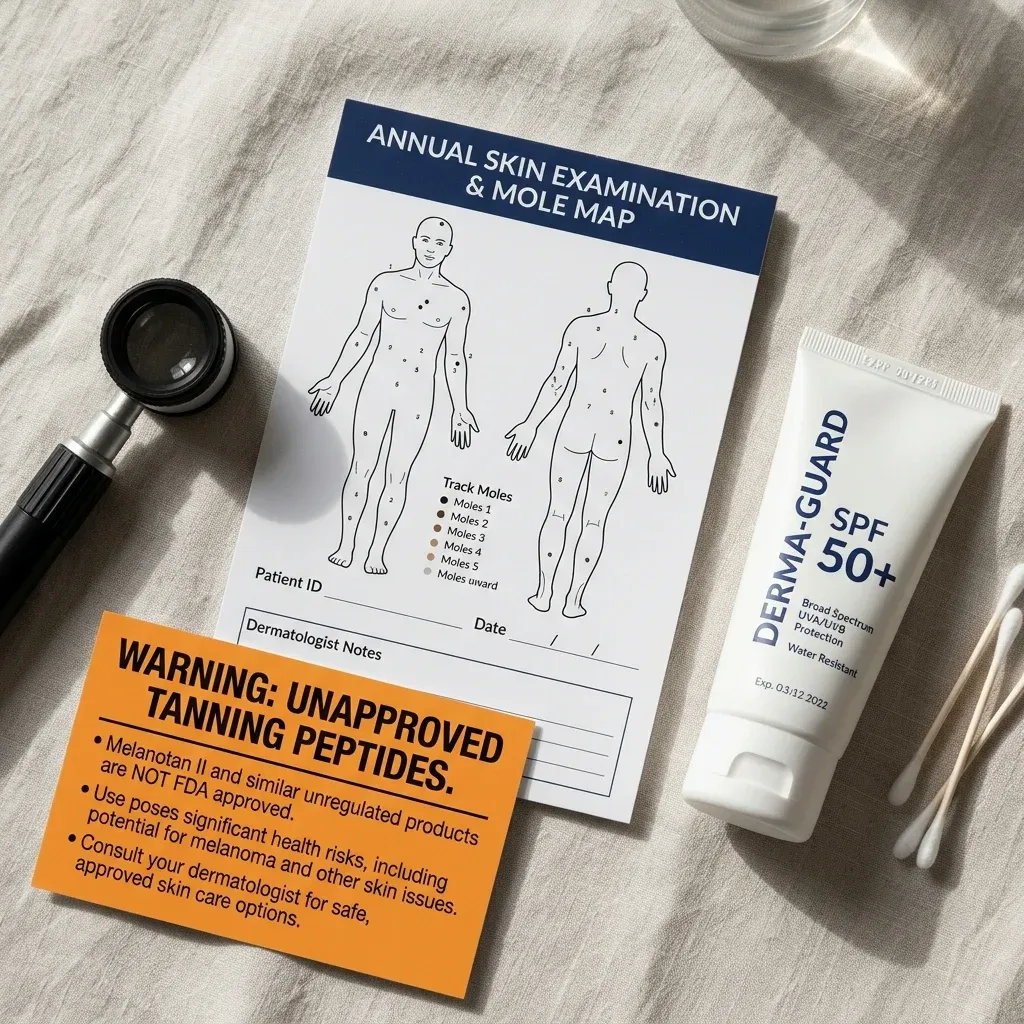
The Therapeutic Goods Administration warns that tanning products containing melanotan are illegally promoted and sold online, are not approved for sale or use as tanning agents in Australia, and have not been assessed for quality or safety in its January 2025 safety notice. It also says the most concerning risk is serious skin cancers and that melanotan-II has been linked with reports of increased moles and freckles, kidney dysfunction, and brain swelling in the same warning.
UNSW dermatologist Dr. John Frew explains the mechanism plainly: Melanotan-II stimulates pigment cells, and enough stimulation can cause abnormal proliferation that may jumpstart melanoma progression according to UNSW Sydney. Pigment cells are like dimmer switches in the skin. Melanotan tries to force the switch upward. The concern is what happens when some switches are already faulty.
Professor Bernard Stewart adds the needed caution. Case reports have described melanomas emerging from existing moles during or shortly after Melanotan-II use, but definitive proof of causation has not been established as UNSW reports. That is exactly how careful cancer communication should sound: serious enough to act on, not strong enough to pretend a case report proves population causation.
The case literature still deserves attention. An Actas Dermo-Sifiliograficas report described a 25-year-old man who developed more than 100 melanocytic nevi after a 4-week course of subcutaneous Melanotan II; clinicians removed 10 atypical lesions, and 3 showed severe dysplasia. A separate review found 18 clinical trials and 21 clinical case presentations, while noting that long-term outcomes remain undocumented and causality is limited by case reporting.
If someone has used melanotan and notices new, changing, bleeding, itching, or unusually dark moles, the next step is not online debate. It is a skin exam. Compared with other peptide categories, melanotan has the clearest practical message: avoid unapproved tanning peptides, and do not treat a darker tan as protection from ultraviolet damage.
BPC-157 and Angiogenesis Claims Are Mostly Theoretical
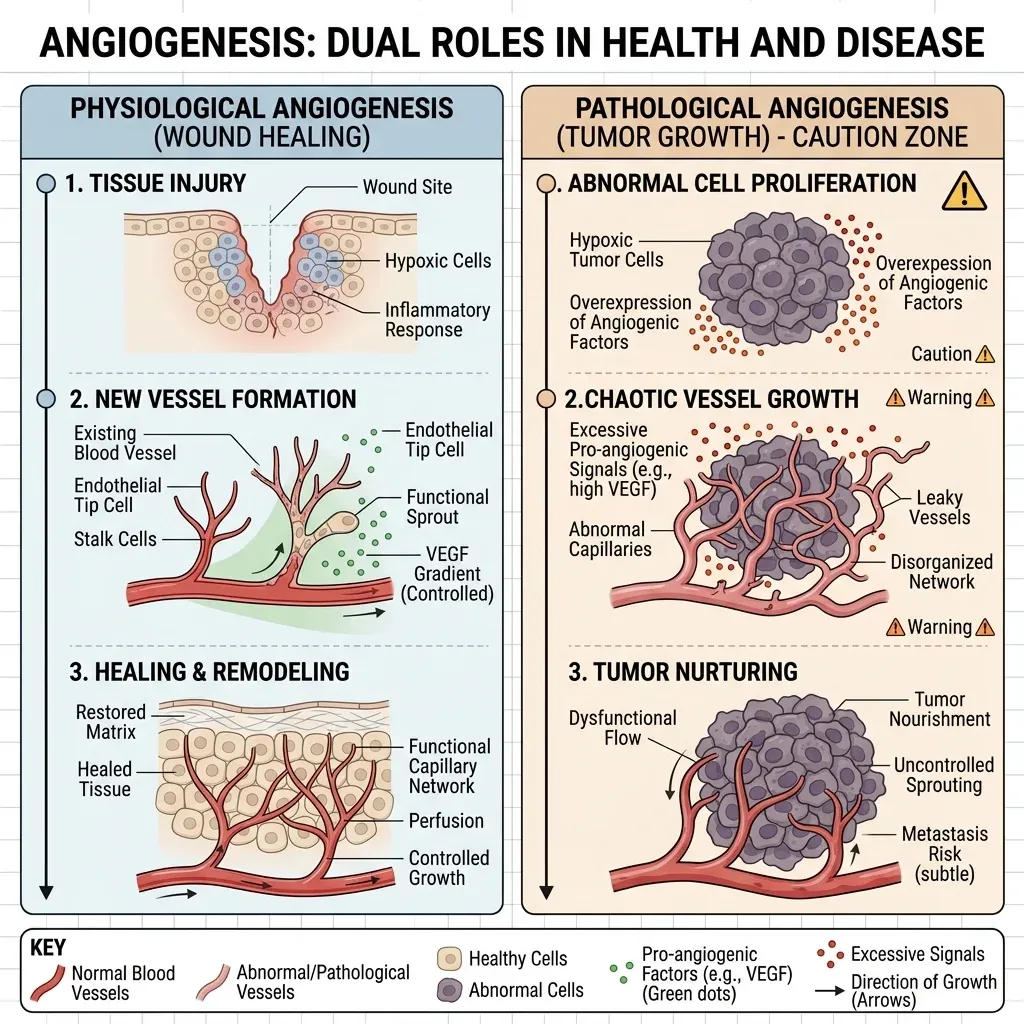
BPC-157 is usually sold with a healing story. The cancer concern comes from the same story: repair, new blood vessels, growth signals, and tissue remodeling. These are useful processes when an injury needs repair. They are also processes cancer biology can exploit.
A Columbia Undergraduate Science Journal article describes BPC-157 as a 15-amino-acid segment of body protection compound and notes that preclinical rat studies have shown it can induce angiogenesis, the formation of new blood vessels. Angiogenesis is like adding roads to a city. After a storm, more roads help emergency crews arrive. Around a tumor, new roads can help supply growth.
The key word is "can," not "does in humans." A narrative review in the American Journal of Sports Medicine says BPC-157's tendon and muscle repair findings are largely unvalidated in human trials in its review of injectable peptide therapy. The same review says TB-4 and TB-500 promoted angiogenesis and tissue repair in preclinical models, but human orthopaedic data are lacking for those peptides as well.
The FDA's position is narrower and more useful than most internet arguments. For BPC-157, the agency says compounded products may pose immunogenicity risks and peptide impurity or API characterization concerns, and that it has no or limited safety-related information for proposed routes of administration in the withdrawn-nominations section. For TB-500, the FDA says it has not identified human exposure data for drug products containing thymosin beta-4 fragment and lacks important safety information in the same table.
| Claim people hear | What the evidence actually supports | Plain-language conclusion |
|---|---|---|
| BPC-157 heals tissue | Promising animal and preclinical signals, weak human evidence | Not enough to assume long-term human safety |
| Angiogenesis is good | It can help repair; tumors also use blood-vessel growth | Mechanism supports caution, not proof of cancer causation |
| TB-500 helps recovery | Preclinical tissue-repair signals, lacking human orthopaedic data | Safety claims are ahead of evidence |
That leaves a careful middle. The current evidence does not show that BPC-157 causes cancer in humans. It also does not justify confident reassurance, especially for people with active cancer, recent remission, unexplained masses, or high-risk lesions. A mechanism that encourages repair should be studied before it is normalized as a wellness injection.
What Clinicians Can and Cannot Conclude
A clinician cannot responsibly answer "Do peptides cause cancer?" without asking which peptide. The evidence points to a category-by-category answer.
For GLP-1 receptor agonists, clinicians can say that current trial and meta-analysis data do not show a broad cancer-risk increase and may show lower risk for some obesity-related cancers. They should also explain that association is not causation, that thyroid signals remain under study, and that longer cancer-specific follow-up is still needed as the obesity-related cancer meta-analysis states.
For tesamorelin, clinicians have label-based guardrails. Active malignancy is a contraindication, recurrent malignancy is a reason to stop, and IGF-1 monitoring is part of the safety logic according to the EGRIFTA WR prescribing information.
For melanotan, clinicians can be more direct. Regulators and dermatology sources describe serious skin-cancer concerns, mole changes, and unapproved online products. They still should not say case reports prove causation. The stronger and more defensible advice is to avoid unapproved tanning peptides and seek medical review for new or changing lesions.
For BPC-157, TB-500, CJC-1295, and ipamorelin, clinicians can say the human safety evidence is thin, product quality is a real concern, and mechanisms such as growth signaling or angiogenesis deserve caution. They cannot honestly say the fetched evidence proves these compounds cause human cancer. They also cannot honestly say they are cancer-safe.
That may feel unsatisfying, but it is the actual science. Cancer risk is rarely a yes-or-no label. It is a map of evidence strength, mechanism, dose, duration, product quality, personal cancer history, and monitoring. Anyone considering a peptide should bring that map to a licensed clinician, especially with a current cancer diagnosis, a history of cancer, unusual moles, unexplained weight loss, or a mass that has not been evaluated.
Frequently Asked Questions
Do GLP-1 medicines like semaglutide cause cancer?
Current human data do not show a broad cancer-risk increase. A 50-trial meta-analysis found no significant difference in overall cancer risk, while a thyroid signal remains under study. People with a personal or family history of medullary thyroid cancer should follow their clinician's prescribing guidance.
Is melanotan different from other peptides?
Yes. Melanotan directly stimulates pigment biology, is sold online as an unapproved tanning product, and has regulator warnings plus case reports involving mole changes and melanoma concerns from the TGA. It is one of the clearest avoid categories.
Does BPC-157 cause cancer?
The fetched evidence does not prove that BPC-157 causes cancer in humans. The stronger conclusion is that BPC-157 has preclinical growth and angiogenesis signals, limited human safety data, and FDA compounding concerns for BPC-157 products.
Should cancer survivors avoid all peptides?
Not automatically, but cancer survivors should not self-start research or wellness peptides. Some approved peptide medicines may be appropriate under medical supervision, while growth-hormone-axis peptides require extra caution because labels such as EGRIFTA WR directly address malignancy and IGF-1 monitoring in the prescribing information.
What should I ask before using any peptide?
Ask whether it is FDA-approved for your condition, whether human safety data exist, whether the product source is regulated, what monitoring is needed, and whether your personal cancer history changes the risk-benefit calculation.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











