
A peptide can look harmless because the dose is tiny, the vial is small, and the marketing often sounds more like wellness than medicine. That is exactly why interactions get missed. FDA-approved peptide drugs, GLP-1 medicines, tesamorelin, and research peptides do not all behave the same way, but they can all collide with a patient’s real medication list in ways that matter.
The safest starting point is boring: treat every peptide like a drug until your clinician says otherwise. A peptide prescription, a compounded version, a research vial, and a supplement-like product may sit in the same online conversation, but they do not carry the same evidence. The FDA says compounded drugs are not FDA-approved and that the agency does not verify their safety, effectiveness, or quality before marketing, while Health Canada warns that unauthorized injectable peptide drugs have not been assessed for safety, efficacy, or quality and may expose users to risks including blood sugar imbalance, blood clots, and tumor growth according to FDA compounding guidance and Health Canada’s peptide warning.
Why peptide interactions are easy to miss
Most people think of drug interactions as a liver-enzyme problem: one pill blocks the metabolism of another pill, blood levels rise, and a warning pops up at the pharmacy. Peptides can be trickier. Some are degraded into amino acids. Some act through hormones. Some slow the stomach. Some change immune signaling. Think of it less like two cars trying to use the same lane, and more like one medicine changing the traffic lights across town.
The FDA’s draft guidance on peptide drug products specifically includes drug-drug interactions, hepatic impairment, QTc risk, and immunogenicity as clinical pharmacology issues that developers should evaluate in peptide drug products. That matters because “peptide” is not one interaction category. Semaglutide, tirzepatide, tesamorelin, thymosin-alpha-1, and gray-market growth-hormone secretagogues raise different questions.
If the product is FDA-approved, start with the label. If it is compounded or sold as a research peptide, assume the interaction evidence is thinner, not safer.
This distinction is especially important with compounded and unauthorized products. FDA says bulk drug substances used in compounding may present significant safety risks, and its list includes several peptide-related substances such as GHRP-2, GHRP-6, CJC-1295, ipamorelin, AOD-9604, and thymosin-alpha-1 in its safety-risk review. That does not prove a specific interaction with every prescription drug. It means the honest answer is often, “we do not have enough monitored human data.”
| Peptide category | Interaction question doctors care about | Evidence posture |
|---|---|---|
| GLP-1 and GIP/GLP-1 drugs | Delayed stomach emptying, oral drug timing, hypoglycemia with insulin or sulfonylureas | FDA labels and clinical pharmacology data |
| Tesamorelin | Glucocorticoid replacement, CYP450-metabolized drugs, diabetes, malignancy history | FDA label data and interaction studies |
| Research or compounded peptides | Unknown safety, immunogenicity, blood sugar effects, product quality | Regulatory warnings, limited or absent clinical data |
Practically, this means your clinician needs more than the peptide name. They need the exact product, route, dose, source, start date, and the full medication list. A vague “I’m on peptides” is like telling a pharmacist you take “heart medicine.” It points in the right direction, but it is not enough to keep you safe.
GLP-1 medications can change the timing of oral drugs
GLP-1 medications are the interaction category many patients underestimate. Semaglutide labels say these drugs delay gastric emptying and may affect absorption of oral medicines in the oral semaglutide label. The practical analogy is a train station: the medicine may still arrive, but the platform timing changes. For many drugs, that shift is not clinically important. For a few, timing and peak levels matter.
Levothyroxine is the cleanest example. Oral semaglutide increased total thyroxine exposure by 33% when administered with levothyroxine. That does not mean everyone on thyroid medicine must stop GLP-1 therapy. It means thyroid labs and symptoms deserve attention when oral semaglutide enters the picture, especially because levothyroxine has a narrow dosing window.
Injectable semaglutide is more reassuring but not consequence-free. Ozempic and Wegovy labeling reports no clinically relevant absorption change for evaluated oral medicines in clinical pharmacology trials, while still warning that delayed gastric emptying may affect concomitantly administered oral medications in the Ozempic label and in the Wegovy label. That nuance is the part patients miss: “usually okay” is not the same as “ignore your medication list.”
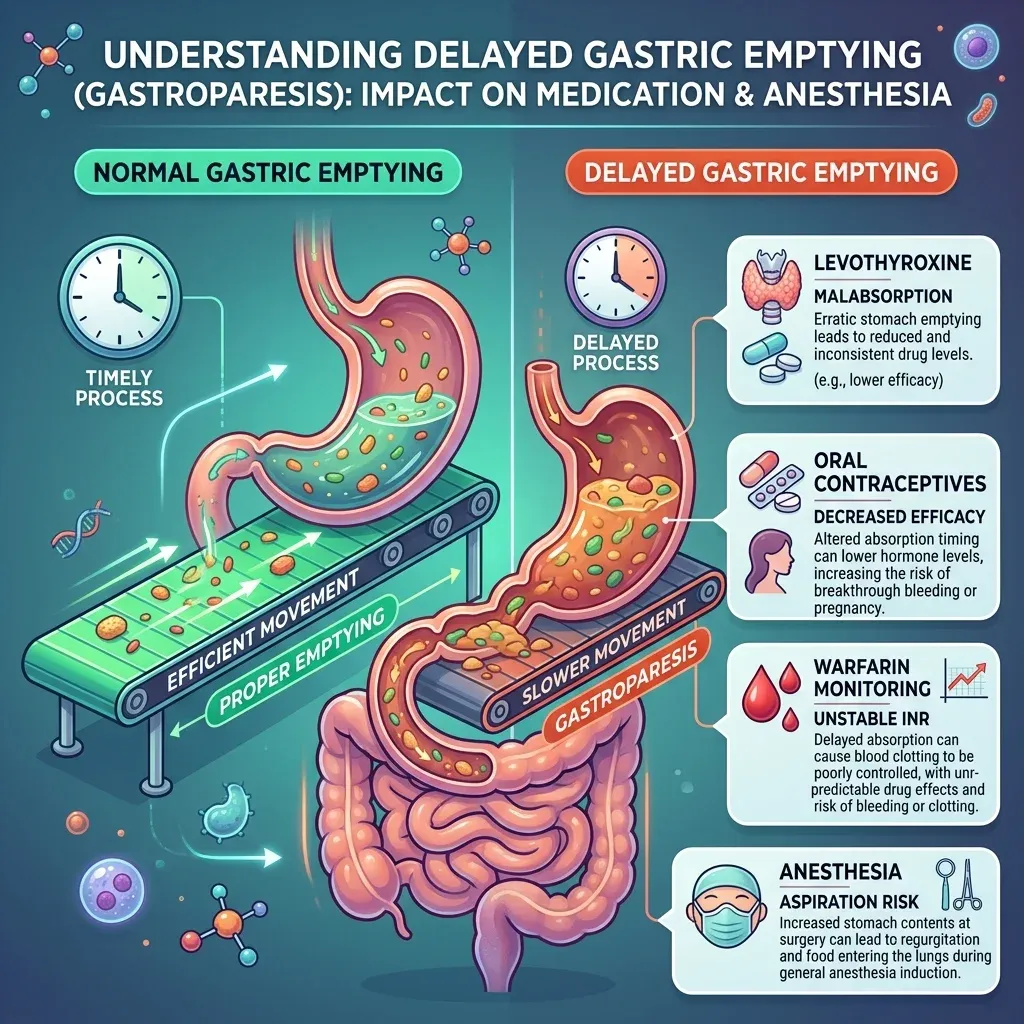
Tirzepatide raises a different warning for oral hormonal contraceptives. The Mounjaro label advises patients using oral hormonal contraceptives to switch to a non-oral method or add a barrier method for 4 weeks after initiation and 4 weeks after each dose escalation. The label also says to monitor oral drugs that depend on threshold concentrations, including narrow-therapeutic-index drugs such as warfarin when used with Mounjaro.
The practical takeaway is simple: if a pill must work at a specific blood level, ask before starting or increasing a GLP-1 drug. Thyroid replacement, oral contraception, warfarin, seizure medicines, transplant medicines, and some psychiatric medicines deserve a more careful conversation than a multivitamin.
Blood sugar drugs need extra attention
The most immediate interaction risk is not exotic. It is low blood sugar. Ozempic labeling warns that use with insulin or insulin secretagogues such as sulfonylureas may increase hypoglycemia risk, including severe hypoglycemia, and that lowering the insulin or secretagogue dose may reduce that risk according to the Ozempic prescribing information.
This is not because semaglutide acts like insulin. Semaglutide stimulates insulin secretion and lowers glucagon secretion in a glucose-dependent manner as described in its clinical pharmacology section. Add it to medicines that already push glucose down, and the safety margin narrows. Think of blood sugar like a thermostat controlled by several hands at once. A small adjustment from one hand may be fine until two other hands turn the dial at the same time.
Diabetes Canada guidance says hypoglycemia caused by insulin or insulin secretagogues can be distressing and potentially debilitating, and it recommends reassessing the dose and need for those agents at each clinic visit in high-risk patients in its hypoglycemia guidance. That is the kind of practical monitoring that gets lost when a peptide is started outside the clinician who manages diabetes medication.

| Medication combination | Main concern | Clinician question |
|---|---|---|
| GLP-1 plus insulin | Hypoglycemia, including severe hypoglycemia | Should insulin dose or glucose monitoring change? |
| GLP-1 plus sulfonylurea | Too much insulin secretory pressure | Should the secretagogue dose be reduced? |
| GH-related peptide plus diabetes medicine | Possible higher glucose or insulin resistance | Do fasting glucose, A1c, or home readings need closer review? |
Growth-hormone secretagogues point in the opposite direction. FDA’s safety-risk page says GHRP-6 has concerns including possible cortisol effects and increased blood glucose due to decreased insulin sensitivity, while a review of growth-hormone secretagogues notes concern for increased blood glucose because of decreased insulin sensitivity in FDA’s compounding review and in a GHS safety review. That does not prove every GH peptide will derail diabetes control. It does mean patients on diabetes medicines should not treat these products as metabolically neutral.
If you use insulin, a sulfonylurea, or any medicine where low glucose is a real possibility, the first call should be to the prescriber managing your diabetes. Bring glucose logs. Bring the exact peptide name. Do not wait for fainting, night sweats, confusion, or rebound overeating to tell you the combination was too strong.
Growth-hormone related peptides raise different flags
Tesamorelin is a useful example because it is an FDA-approved peptide with a real label, not a rumor. The label is explicit: active malignancy is a contraindication, and any preexisting malignancy should be inactive with treatment complete before starting Egrifta SV. That is not a typical “drug interaction,” but doctors think about it in the same visit because growth-hormone signaling can change the risk-benefit calculation.
The glucose warning is also direct. Tesamorelin can cause glucose intolerance or diabetes, and the label says to evaluate glucose before and during therapy in the prescribing information. For someone already taking metformin, insulin, a sulfonylurea, or a GLP-1 drug, that becomes a medication-management issue, not a cosmetic footnote.
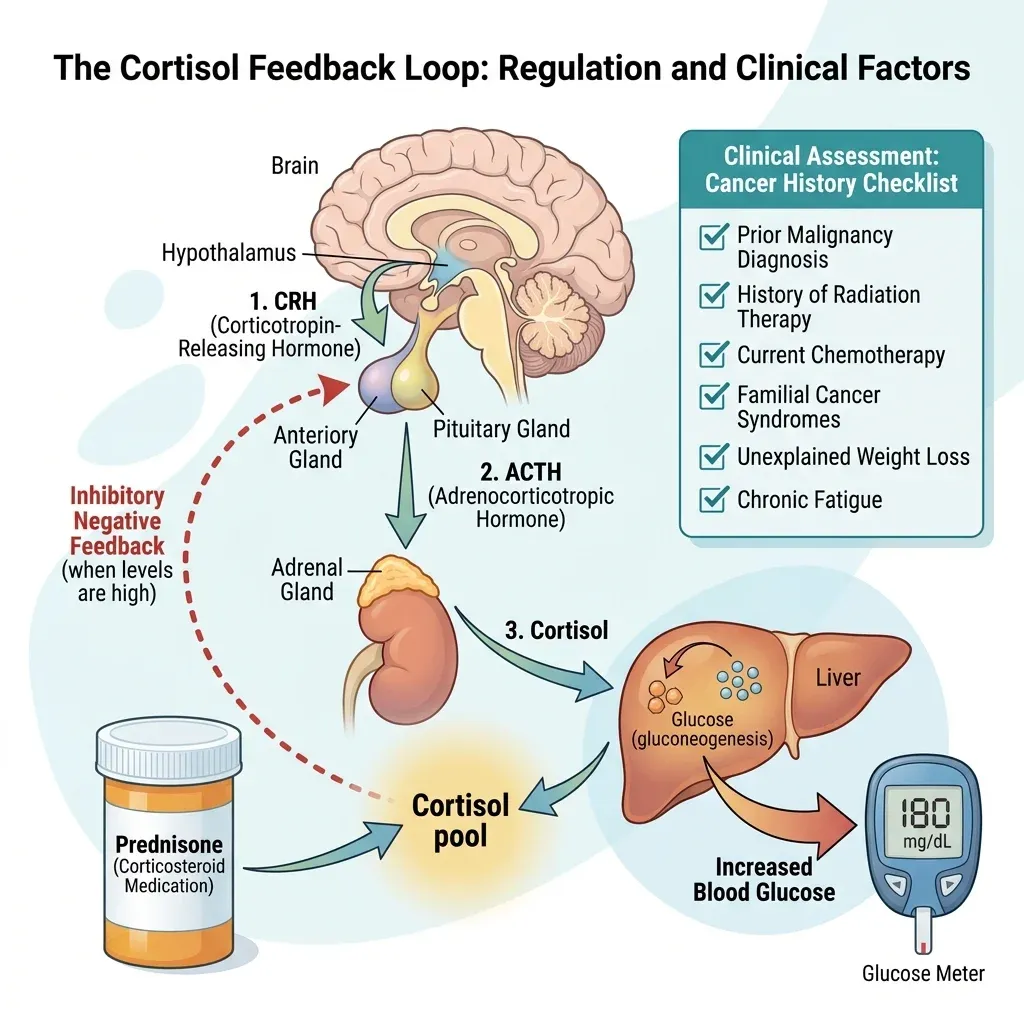
The steroid interaction is one doctors particularly care about. Tesamorelin labels say growth hormone may alter clearance of CYP450-metabolized drugs such as corticosteroids, sex steroids, anticonvulsants, and cyclosporine, and patients taking glucocorticoid replacement for hypoadrenalism may need higher maintenance or stress doses after starting tesamorelin according to Egrifta SV labeling. Put plainly: if your adrenal replacement plan is carefully balanced, a GH-releasing peptide can move the floor under it.
There are measured pharmacokinetic findings too. Tesamorelin coadministration decreased ritonavir AUC and Cmax by 9% and 11%, and Liverpool HIV Interactions considered those changes not clinically relevant. In healthy subjects, tesamorelin with simvastatin resulted in an 8% decrease in simvastatin AUC and a 5% increase in Cmax. These numbers are modest, but they illustrate the broader point: “peptide” does not mean “no interaction study needed.”
| Growth-hormone related issue | What the source says | Why it changes the visit |
|---|---|---|
| Tesamorelin and glucocorticoids | Replacement doses may need maintenance or stress-dose increases | Adrenal plans need clinician review |
| Tesamorelin and glucose | Glucose intolerance or diabetes may develop | Diabetes medicines and labs may need adjustment |
| GHRP-6 and glucose | FDA notes increased blood glucose concerns from decreased insulin sensitivity | Research-peptide use should not be hidden from diabetes care |
For non-approved GH secretagogues, the evidence gets thinner and the warnings get less tidy. FDA says GHRP-2 reports included increased insulin requirement, death of critically ill study subjects, infection, and pancreatitis, while noting causality was not established in its compounding safety-risk list. FDA also says ibutamoren mesylate poses significant safety risks because a randomized trial was terminated early after a potential congestive heart failure signal in the same review. The practical implication is not “never discuss these.” It is “do not force your doctor to guess.”
Immune, surgery, and cancer cautions
Some interaction-like cautions are not about blood levels. Surgery is one. Semaglutide labels say pulmonary aspiration has been reported in patients taking GLP-1 receptor agonists during procedures requiring general anesthesia or deep sedation, even with reported adherence to preoperative fasting in Ozempic labeling. Tirzepatide carries similar language and tells patients to inform healthcare providers before planned procedures in the Mounjaro label.
This is not a reason to panic before every dental cleaning. It is a reason to tell the anesthesia team. Delayed gastric emptying is like a dishwasher cycle that runs longer than expected: the clock says it should be empty, but there may still be contents inside. The label says available data are insufficient to know whether changing fasting instructions or temporarily stopping the medicine reduces aspiration risk for Ozempic, so the decision belongs with the procedural team, not a social media dosing calendar.
Cancer history is another category that patients often mislabel as a side effect instead of a prescribing boundary. Semaglutide products are contraindicated for people with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 in Rybelsus and Ozempic tablet labeling. Tesamorelin is contraindicated in active malignancy and should be stopped if there is evidence of recurrent malignancy according to Egrifta SV labeling.
Immune-modulating peptides require even more humility. A PubMed-indexed rat study found recombinant human thymosin-alpha1 modulated rat CYP isoforms, but the authors said further studies were needed to investigate human CYP activity and interaction potential in the PubMed abstract. FDA also says compounded thymosin-alpha-1 may carry immunogenicity and impurity-characterization risks, and that available safety information is inadequate in its bulk-substance review.
The same caution applies to anticoagulants. The strongest sourced point here is not that every peptide interacts with blood thinners. It is that tirzepatide labeling calls out threshold-dependent oral drugs and narrow-therapeutic-index drugs such as warfarin for monitoring when used with Mounjaro. For other research peptides, a precise anticoagulant interaction list would be false confidence. If you take warfarin, apixaban, rivaroxaban, clopidogrel, aspirin for a medical reason, or have surgery planned, tell the clinician before adding a peptide.
What to tell your clinician before starting a peptide
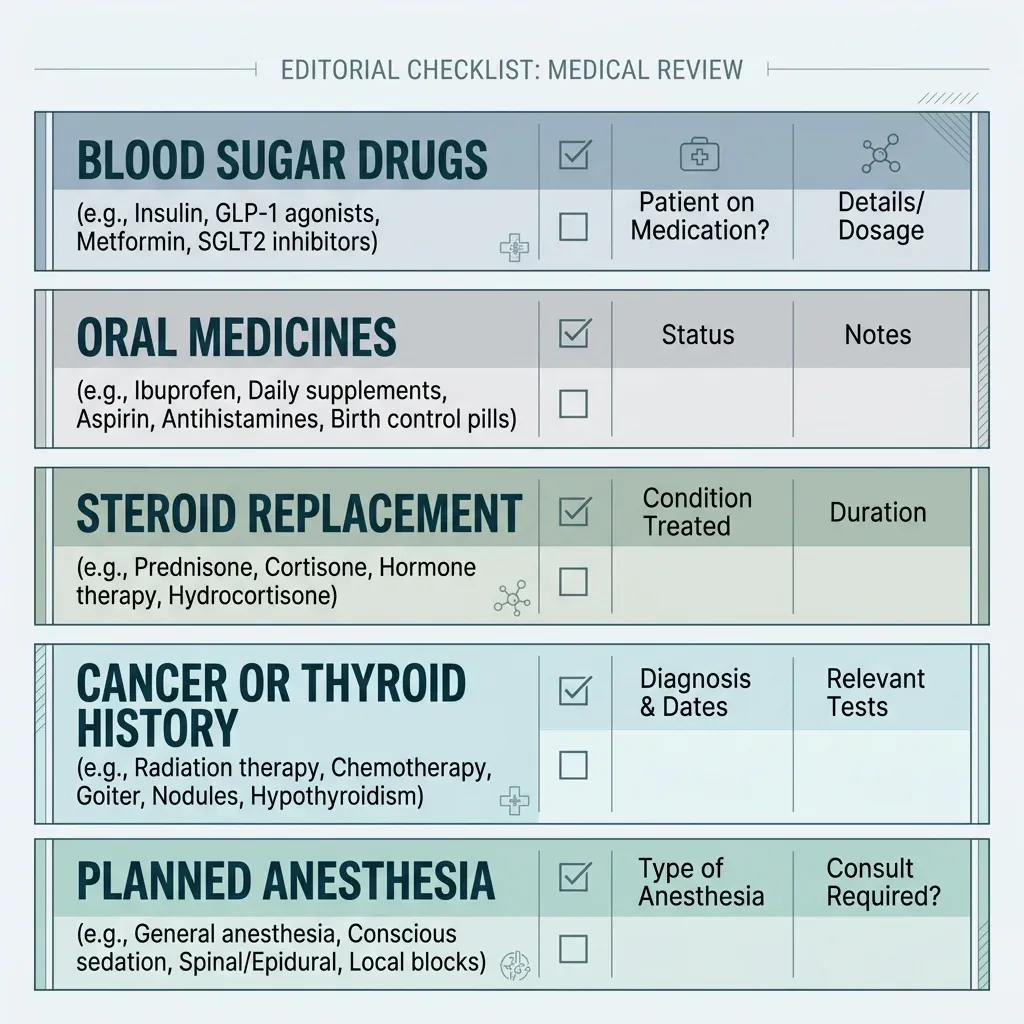
A good peptide-safety visit is not a confession. It is a reconciliation, the same kind pharmacists do before surgery or hospital discharge. Bring the drug name, dose, route, frequency, source, start date, and reason for use. Bring every prescription, over-the-counter medicine, supplement, and injection. The interaction risk is often hiding in the combination.

Use this short checklist before starting, stopping, or increasing a peptide:
- Are you taking insulin, a sulfonylurea, or another medicine that can cause low blood sugar?
- Do you take levothyroxine, oral contraception, warfarin, seizure medicine, transplant medicine, steroids, or any narrow-therapeutic-index drug?
- Do you have a personal or family history of medullary thyroid carcinoma, MEN 2, active cancer, treated cancer, adrenal insufficiency, diabetes, kidney disease, or severe gastroparesis?
- Are you scheduled for surgery, endoscopy, dental sedation, or any procedure using anesthesia or deep sedation?
- Is the peptide FDA-approved for your indication, compounded by a licensed pharmacy for you, or sold as a research product?
The answer should change the plan. Maybe the plan is lab monitoring. Maybe it is a dose adjustment. Maybe it is a non-oral contraceptive method for a period of time. Maybe it is postponing an unapproved peptide because the risk is unknown. FDA-approved labels repeatedly point clinicians toward monitoring for oral medicines, narrow-therapeutic-index drugs, diabetes medicines, glucocorticoids, planned procedures, malignancy history, and thyroid cancer history in semaglutide labeling, tirzepatide labeling, and tesamorelin labeling.
The most conservative rule is also the most useful: do not invent certainty. If a peptide is unapproved, compounded from a substance FDA has flagged, or purchased online without medical oversight, the interaction profile may be unknown rather than reassuring. Unknown is a real clinical answer. It is also a reason to slow down.
Frequently Asked Questions
Can GLP-1 medications make my other pills stop working?
Usually not in a dramatic way, but some drugs deserve monitoring. Semaglutide labels say delayed gastric emptying may affect oral medication absorption, while oral semaglutide increased levothyroxine exposure by 33%. Tirzepatide labeling also gives specific contraception advice.
Should I stop my GLP-1 before surgery?
Do not decide alone. GLP-1 labels report pulmonary aspiration during anesthesia or deep sedation and say data are insufficient to know whether changing fasting or temporarily stopping the drug reduces risk according to Ozempic labeling. Tell the anesthesia or procedural team early.
Are research peptides safer because they are not regular drugs?
No. FDA has flagged several peptide-related bulk substances for potential significant safety risks, and Health Canada warns that unauthorized injectable peptides have not been assessed for safety, efficacy, or quality in FDA’s review and Health Canada’s warning.
What if my doctor does not know much about peptides?
Give them the exact product and ask them to check the medication risks they do know: glucose-lowering drugs, thyroid medicine, contraception, anticoagulants, steroids, immune medicines, cancer history, and anesthesia plans. A pharmacist or specialist can help when the peptide itself is unfamiliar.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











